Paules Catharine I, Nordwall Jacqueline A, Shaw-Saliba Kathryn, Aberg Judith A, Gardner Edward M, Goodman Anna L, Kumarasamy N, Vasudeva Shikha, Vock David M, North Crystal M, Lundgren Jens, Aggarwal Neil R
Division of Infectious Diseases, Penn State Health Milton S. Hershey Medical Center, 500 University Drive, Hershey, PA, 17033, USA.
Division of Biostatistics and Health Data Science, School of Public Health, University of Minnesota, Minneapolis, MN, USA.
BMC Infect Dis. 2025 Jan 15;25(1):67. doi: 10.1186/s12879-024-10428-7.
Low blood absolute lymphocyte count (ALC) may predict severe COVID-19 outcomes. Knowledge gaps remain regarding the relationship of ALC trajectory with clinical outcomes and factors associated with lymphopenia.
Our post hoc analysis of the Therapeutics for Inpatients with COVID-19 platform trial utilized proportional hazards models to assess relationships between Day (D) 0 lymphopenia (ALC < 0.9 cells/uL), D0 severe lymphopenia (ALC < 0.5 cells/uL) or lymphopenia trajectory between D0 and D5 with mortality and secondary infections, and with sustained recovery using Fine-Gray models. Logistic regression was used to assess relationships between clinical variables and D0 lymphopenia or lymphopenia trajectory.
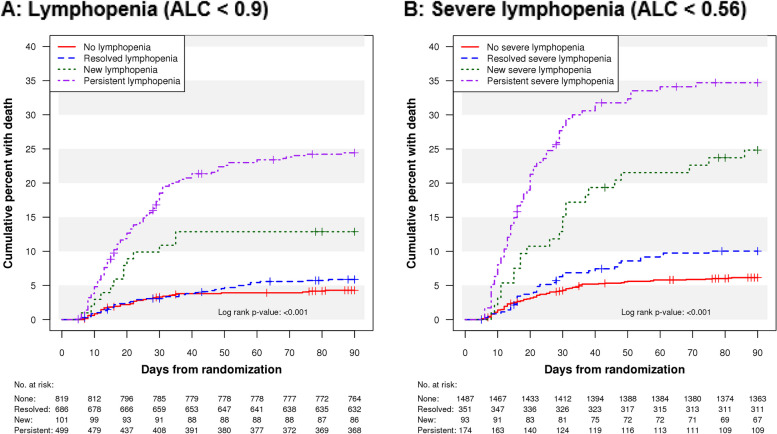
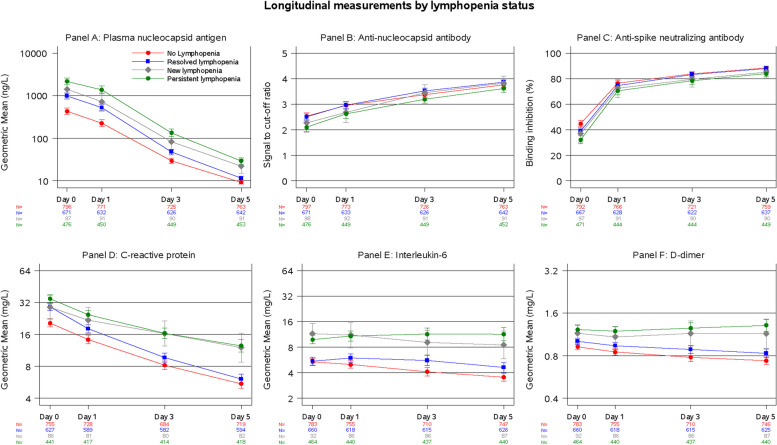
D0 lymphopenia (1426/2579) and severe lymphopenia (636/2579) were associated with increased mortality (aHR 1.48; 1.08, 2.05, p = 0.016 and aHR 1.60; 1.20, 2.14, p = 0.001) and decreased recovery (aRRR 0.90; 0.82, 0.99, p = 0.033 and aRRR 0.78; 0.70, 0.87, p < 0.001 respectively). Trial participants with persistent D5 lymphopenia had increased mortality, and increased secondary infections, and participants with persistent or new lymphopenia had impaired recovery, as compared to participants with no lymphopenia. Persistent and new lymphopenia were associated with older age, male sex; prior immunosuppression, heart failure, aspirin use, and normal body mass index; biomarkers of organ damage (renal and lung), and ineffective immune response (elevated IL-6 and viral nucleocapsid antigen levels). Similar results were observed with severe lymphopenia.
Lymphopenia was predictive of severe COVID-19 outcomes, particularly when persistent or new during hospitalization. A better understanding of the underlying risk factors for lymphopenia will help illuminate disease pathogenesis and guide management strategies.
低血液绝对淋巴细胞计数(ALC)可能预测新冠肺炎的严重结局。关于ALC轨迹与临床结局以及淋巴细胞减少相关因素之间的关系仍存在知识空白。
我们对新冠肺炎住院患者治疗平台试验的事后分析使用比例风险模型来评估第0天淋巴细胞减少(ALC<0.9细胞/微升)、第0天严重淋巴细胞减少(ALC<0.5细胞/微升)或第0天至第5天之间的淋巴细胞减少轨迹与死亡率和继发感染之间的关系,以及使用Fine-Gray模型评估与持续恢复之间的关系。采用逻辑回归评估临床变量与第0天淋巴细胞减少或淋巴细胞减少轨迹之间的关系。
第0天淋巴细胞减少(1426/2579)和严重淋巴细胞减少(636/2579)与死亡率增加(风险比1.48;1.08,2.05,p = 0.016和风险比1.60;1.20,2.14,p = 0.001)和恢复率降低(绝对风险降低率0.90;0.82,0.99,p = 并0.033和绝对风险降低率0.78;0.70,0.87,p分别<0.001)相关。与无淋巴细胞减少的参与者相比,持续第5天淋巴细胞减少的试验参与者死亡率增加,继发感染增加,持续或新发淋巴细胞减少的参与者恢复受损。持续和新发淋巴细胞减少与年龄较大、男性、既往免疫抑制、心力衰竭、使用阿司匹林以及正常体重指数、器官损伤生物标志物(肾脏和肺部)和无效免疫反应(白细胞介素-6和病毒核衣壳抗原水平升高)相关。严重淋巴细胞减少也观察到类似结果。
淋巴细胞减少可预测新冠肺炎的严重结局,尤其是在住院期间持续存在或新发时。更好地了解淋巴细胞减少的潜在危险因素将有助于阐明疾病发病机制并指导管理策略。