Division of Gastroenterology, Veterans Affairs Puget Sound Healthcare System and University of Washington, Seattle.
Research and Development, Veterans Affairs Puget Sound Health Care System, Seattle, Washington.
JAMA Netw Open. 2020 Sep 1;3(9):e2022310. doi: 10.1001/jamanetworkopen.2020.22310.
Identifying independent risk factors for adverse outcomes in patients infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) can support prognostication, resource utilization, and treatment.
To identify excess risk and risk factors associated with hospitalization, mechanical ventilation, and mortality in patients with SARS-CoV-2 infection.
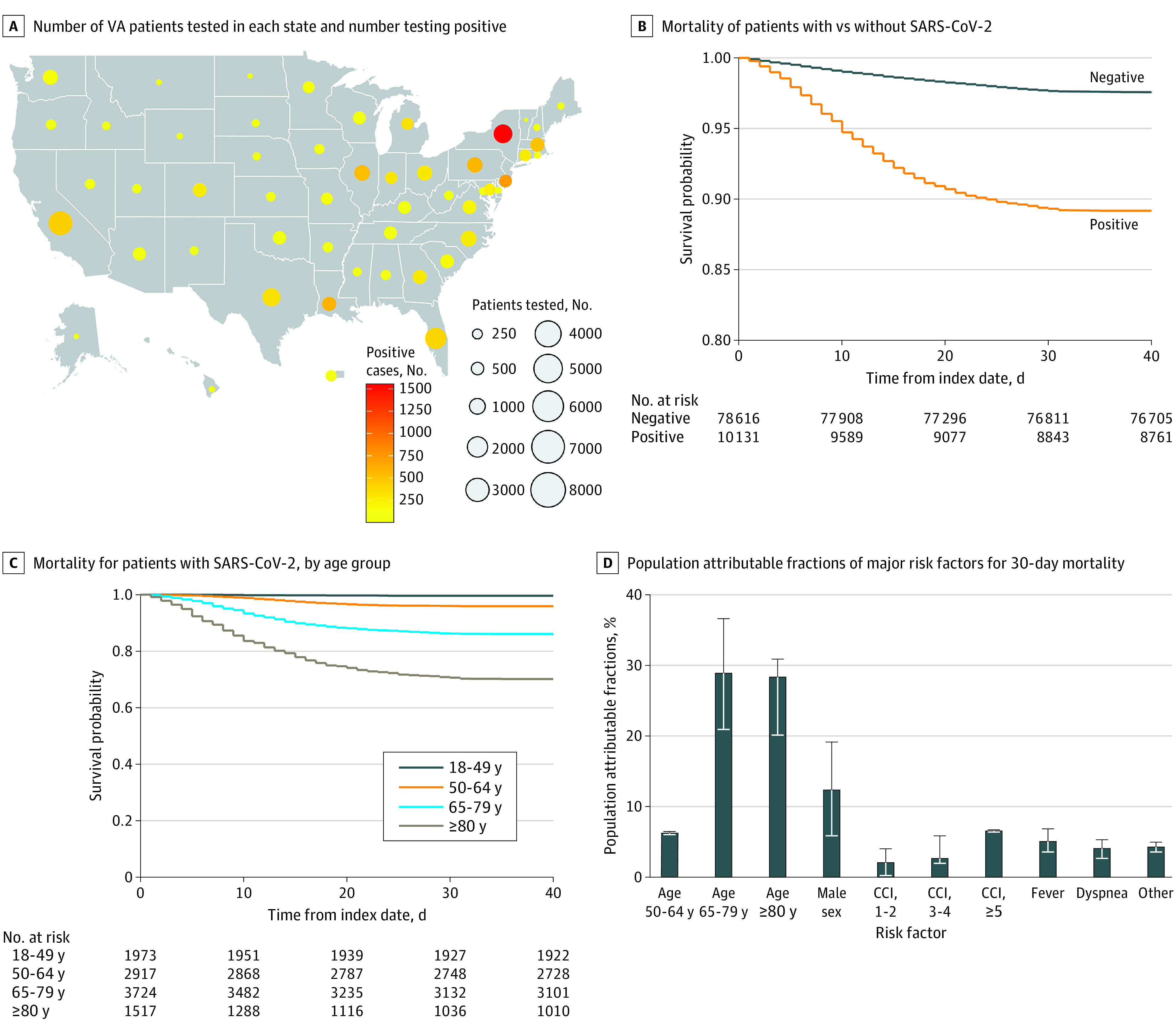
DESIGN, SETTING, AND PARTICIPANTS: This longitudinal cohort study included 88 747 patients tested for SARS-CoV-2 nucleic acid by polymerase chain reaction between Feburary 28 and May 14, 2020, and followed up through June 22, 2020, in the Department of Veterans Affairs (VA) national health care system, including 10 131 patients (11.4%) who tested positive.
Sociodemographic characteristics, comorbid conditions, symptoms, and laboratory test results.
Risk of hospitalization, mechanical ventilation, and death were estimated in time-to-event analyses using Cox proportional hazards models.
The 10 131 veterans with SARS-CoV-2 were predominantly male (9221 [91.0%]), with diverse race/ethnicity (5022 [49.6%] White, 4215 [41.6%] Black, and 944 [9.3%] Hispanic) and a mean (SD) age of 63.6 (16.2) years. Compared with patients who tested negative for SARS-CoV-2, those who tested positive had higher rates of 30-day hospitalization (30.4% vs 29.3%; adjusted hazard ratio [aHR], 1.13; 95% CI, 1.08-1.13), mechanical ventilation (6.7% vs 1.7%; aHR, 4.15; 95% CI, 3.74-4.61), and death (10.8% vs 2.4%; aHR, 4.44; 95% CI, 4.07-4.83). Among patients who tested positive for SARS-CoV-2, characteristics significantly associated with mortality included older age (eg, ≥80 years vs <50 years: aHR, 60.80; 95% CI, 29.67-124.61), high regional COVID-19 disease burden (eg, ≥700 vs <130 deaths per 1 million residents: aHR, 1.21; 95% CI, 1.02-1.45), higher Charlson comorbidity index score (eg, ≥5 vs 0: aHR, 1.93; 95% CI, 1.54-2.42), fever (aHR, 1.51; 95% CI, 1.32-1.72), dyspnea (aHR, 1.78; 95% CI, 1.53-2.07), and abnormalities in the certain blood tests, which exhibited dose-response associations with mortality, including aspartate aminotransferase (>89 U/L vs ≤25 U/L: aHR, 1.86; 95% CI, 1.35-2.57), creatinine (>3.80 mg/dL vs 0.98 mg/dL: aHR, 3.79; 95% CI, 2.62-5.48), and neutrophil to lymphocyte ratio (>12.70 vs ≤2.71: aHR, 2.88; 95% CI, 2.12-3.91). With the exception of geographic region, the same covariates were independently associated with mechanical ventilation along with Black race (aHR, 1.52; 95% CI, 1.25-1.85), male sex (aHR, 2.07; 95% CI, 1.30-3.32), diabetes (aHR, 1.40; 95% CI, 1.18-1.67), and hypertension (aHR, 1.30; 95% CI, 1.03-1.64). Notable characteristics that were not significantly associated with mortality in adjusted analyses included obesity (body mass index ≥35 vs 18.5-24.9: aHR, 0.97; 95% CI, 0.77-1.21), Black race (aHR, 1.04; 95% CI, 0.88-1.21), Hispanic ethnicity (aHR, 1.03; 95% CI, 0.79-1.35), chronic obstructive pulmonary disease (aHR, 1.02; 95% CI, 0.88-1.19), hypertension (aHR, 0.95; 95% CI, 0.81-1.12), and smoking (eg, current vs never: aHR, 0.87; 95% CI, 0.67-1.13). Most deaths in this cohort occurred in patients with age of 50 years or older (63.4%), male sex (12.3%), and Charlson Comorbidity Index score of at least 1 (11.1%).
In this national cohort of VA patients, most SARS-CoV-2 deaths were associated with older age, male sex, and comorbidity burden. Many factors previously reported to be associated with mortality in smaller studies were not confirmed, such as obesity, Black race, Hispanic ethnicity, chronic obstructive pulmonary disease, hypertension, and smoking.
确定严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2) 感染患者不良结局的独立风险因素可以支持预后、资源利用和治疗。
确定 SARS-CoV-2 感染患者住院、机械通气和死亡的超额风险和风险因素。
设计、地点和参与者:本纵向队列研究纳入了 2020 年 2 月 28 日至 5 月 14 日期间通过聚合酶链反应对 SARS-CoV-2 核酸检测呈阳性的退伍军人事务部 (VA) 国家医疗保健系统的 88747 例患者,随访至 2020 年 6 月 22 日,其中包括 10131 例(11.4%)检测呈阳性的患者。
社会人口统计学特征、合并症、症状和实验室检测结果。
使用 Cox 比例风险模型在时间事件分析中估计住院、机械通气和死亡的风险。
10131 例 SARS-CoV-2 退伍军人主要为男性(9221 [91.0%]),种族/民族多样(5022 [49.6%] 白人、4215 [41.6%] 黑人、944 [9.3%] 西班牙裔),平均(SD)年龄为 63.6(16.2)岁。与 SARS-CoV-2 检测阴性的患者相比,检测阳性的患者 30 天住院率(30.4%比 29.3%;调整后的危险比[HR],1.13;95%CI,1.08-1.13)、机械通气(6.7%比 1.7%;HR,4.15;95%CI,3.74-4.61)和死亡率(10.8%比 2.4%;HR,4.44;95%CI,4.07-4.83)更高。在 SARS-CoV-2 检测阳性的患者中,与死亡率显著相关的特征包括年龄较大(例如,≥80 岁与<50 岁:HR,60.80;95%CI,29.67-124.61)、高区域 COVID-19 疾病负担(例如,≥700 与<130 人/百万人死亡:HR,1.21;95%CI,1.02-1.45)、较高的 Charlson 合并症指数评分(例如,≥5 与 0:HR,1.93;95%CI,1.54-2.42)、发热(HR,1.51;95%CI,1.32-1.72)、呼吸困难(HR,1.78;95%CI,1.53-2.07)和某些血液检测异常,这些异常与死亡率呈剂量反应关系,包括天冬氨酸转氨酶(>89 U/L 与≤25 U/L:HR,1.86;95%CI,1.35-2.57)、肌酐(>3.80 mg/dL 与 0.98 mg/dL:HR,3.79;95%CI,2.62-5.48)和中性粒细胞与淋巴细胞比值(>12.70 与≤2.71:HR,2.88;95%CI,2.12-3.91)。除了地理位置,同样的协变量与机械通气以及黑人种族(HR,1.52;95%CI,1.25-1.85)、男性(HR,2.07;95%CI,1.30-3.32)、糖尿病(HR,1.40;95%CI,1.18-1.67)和高血压(HR,1.30;95%CI,1.03-1.64)独立相关。在调整后的分析中,与死亡率无显著相关性的显著特征包括肥胖(体重指数≥35 与 18.5-24.9:HR,0.97;95%CI,0.77-1.21)、黑人种族(HR,1.04;95%CI,0.88-1.21)、西班牙裔(HR,1.03;95%CI,0.79-1.35)、慢性阻塞性肺疾病(HR,1.02;95%CI,0.88-1.19)、高血压(HR,0.95;95%CI,0.81-1.12)和吸烟(例如,当前与从不:HR,0.87;95%CI,0.67-1.13)。本队列的大多数死亡发生在年龄 50 岁或以上(63.4%)、男性(12.3%)和 Charlson 合并症指数评分至少为 1(11.1%)的患者中。
在这项退伍军人事务部的全国性队列研究中,大多数 SARS-CoV-2 死亡与年龄较大、男性和合并症负担有关。在较小的研究中先前报道与死亡率相关的许多因素,如肥胖、黑人种族、西班牙裔、慢性阻塞性肺疾病、高血压和吸烟,在本研究中并未得到证实。