Boston University School of Public Health, 715 Albany St, Boston, MA, 02118, USA.
Ariadne Labs, 401 Park Dr 3rd Floor, Boston, MA, 02215, USA.
BMC Health Serv Res. 2022 Oct 25;22(1):1284. doi: 10.1186/s12913-022-08680-1.
Strategies selected to implement the WHO's Surgical Safety Checklist (SSC) are key factors in its ability to improve patient safety. Underutilization of implementation frameworks for informing implementation processes hinders our understanding of the checklists' varying effectiveness in different contexts. This study explored the extent to which SSC implementation practices could be assessed through the i-PARIHS framework and examined how it could support development of targeted recommendations to improve SSC implementation in high-income settings.
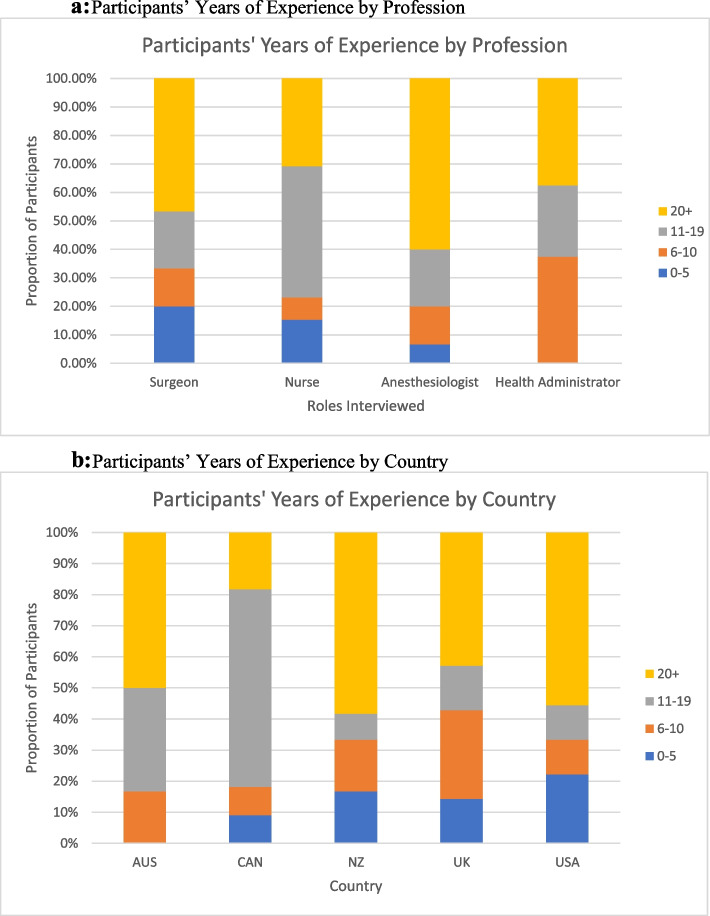
This qualitative study utilized interviews with surgical team members and health administrators from five high-income countries to understand the key elements necessary for successful implementation of the SSC. Using thematic analysis, we identified within and across-case themes that were mapped to the i-PARIHS framework constructs. Gaps in current implementation strategies were identified, and the utility of i-PARIHS to guide future efforts was assessed.
Fifty-one multi-disciplinary clinicians and health administrators completed interviews. We identified themes that impacted SSC implementation in each of the four i-PARIHS constructs and several that spanned multiple constructs. Within innovation, a disconnect between the clinical outcomes-focused evidence in the literature and interviewees' patient-safety focus on observable results reduced the SSC's perceived relevance. Within recipients, existing surgical team hierarchies impacted checklist engagement, but this could be addressed through a shared leadership model. Within context, organizational priorities resulting in time pressures on surgical teams were at odds with SSC patient safety goals and reduced fidelity. At a health system level, employing surgical team members through the state or health region resulted in significant challenges in enforcing checklist use in private vs public hospitals. Within its facilitation construct, i-PARIHS includes limited definitions of facilitation processes. We identified using multiple interdisciplinary champions; establishing checklist performance feedback mechanisms; and modifying checklist processes, such as implementing a full-team huddle, as facilitators of successful SSC implementation.
The i-PARIHS framework enabled a comprehensive assessment of current implementation strategies, identifying key gaps and allowed for recommending targeted improvements. i-PARIHS could serve as a guide for planning future SSC implementation efforts, however, further clarification of facilitation processes would improve the framework's utility.
No health care intervention was performed.
为实施世界卫生组织(WHO)的外科安全检查表(SSC)而选择的策略是提高患者安全性的关键因素。实施框架在告知实施过程方面的利用不足,阻碍了我们了解检查表在不同环境下的不同效果。本研究通过 i-PARIHS 框架探讨了评估 SSC 实施实践的程度,并研究了如何支持制定有针对性的建议,以改善高收入环境中的 SSC 实施。
本定性研究采用对来自五个高收入国家的外科团队成员和卫生行政人员的访谈,以了解成功实施 SSC 的关键要素。使用主题分析,我们确定了与 i-PARIHS 框架结构内和跨案例的主题。确定了当前实施策略中的差距,并评估了 i-PARIHS 对指导未来工作的实用性。
51 名多学科临床医生和卫生行政人员完成了访谈。我们确定了每个 i-PARIHS 结构中影响 SSC 实施的主题,以及几个跨越多个结构的主题。在创新方面,文献中以临床结果为重点的证据与受访者对可观察结果的患者安全重点之间存在脱节,降低了 SSC 的感知相关性。在接受者方面,现有的外科团队层级结构影响了清单的参与度,但可以通过共享领导模式来解决。在背景方面,导致外科团队时间压力的组织优先事项与 SSC 的患者安全目标背道而驰,并降低了一致性。在卫生系统层面,通过州或卫生区域雇用外科团队成员导致在私人与公立医院执行清单使用方面存在重大挑战。在其促进方面,i-PARIHS 包含对促进过程的有限定义。我们确定了使用多个跨学科拥护者;建立清单绩效反馈机制;以及修改清单流程,例如实施全团队围坐会议,作为成功实施 SSC 的促进因素。
i-PARIHS 框架使我们能够全面评估当前的实施策略,确定关键差距,并提出有针对性的改进建议。i-PARIHS 可以作为规划未来 SSC 实施工作的指南,但是,进一步明确促进过程将提高该框架的实用性。
未进行医疗干预。