Kyriakidis Ioannis, Mantadakis Elpis, Stiakaki Eftichia, Groll Andreas H, Tragiannidis Athanasios
Department of Pediatric Hematology-Oncology & Autologous Hematopoietic Stem Cell Transplantation Unit, University Hospital of Heraklion & Laboratory of Blood Diseases and Childhood Cancer Biology, School of Medicine, University of Crete, 70013 Heraklion, Greece.
Department of Paediatrics, Paediatric Hematology/Oncology Unit, Faculty of Medicine, Democritus University of Thrace, 68100 Alexandroupolis, Greece.
Cancers (Basel). 2022 Oct 14;14(20):5022. doi: 10.3390/cancers14205022.
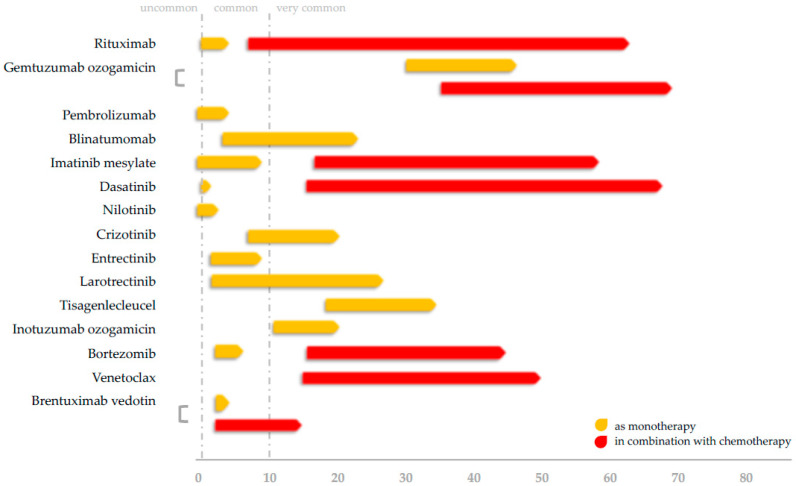
The aim of this review is to highlight mechanisms of immunosuppression for each agent, along with pooled analyses of infectious complications from the available medical literature. Rituximab confers no increase in grade ≥3 infectious risks, except in the case of patients with advanced-stage non-Hodgkin lymphoma. Gemtuzumab ozogamicin links with high rates of grade ≥3 infections which, however, are comparable with historical cohorts. Pembrolizumab exhibits a favorable safety profile in terms of severe infections. Despite high rates of hypogammaglobulinemia (HGG) with blinatumomab, low-grade ≥3 infection rates were observed, especially in the post-reinduction therapy of relapsed B-acute lymphoblastic leukemia. Imatinib and nilotinib are generally devoid of severe infectious complications, but dasatinib may slightly increase the risk of opportunistic infections. Data on crizotinib and pan-Trk inhibitors entrectinib and larotrectinib are limited. CAR T-cell therapy with tisagenlecleucel is associated with grade ≥3 infections in children and is linked with HGG and the emergence of immune-related adverse events. Off-label therapies inotuzumab ozogamicin, brentuximab vedotin, and venetoclax demonstrate low rates of treatment-related grade ≥3 infections, while the addition of bortezomib to standard chemotherapy in T-cell malignancies seems to decrease the infection risk during induction. Prophylaxis, immune reconstitution, and vaccinations for each targeted agent are discussed, along with comparisons to adult studies.
本综述的目的是强调每种药物的免疫抑制机制,并对现有医学文献中的感染并发症进行汇总分析。利妥昔单抗不会增加≥3级感染风险,但晚期非霍奇金淋巴瘤患者除外。吉妥珠单抗奥唑米星与≥3级感染的高发生率相关,不过与历史队列相当。帕博利珠单抗在严重感染方面表现出良好的安全性。尽管贝林妥欧单抗导致低丙种球蛋白血症(HGG)的发生率很高,但观察到≥3级感染率较低,尤其是在复发的B细胞急性淋巴细胞白血病诱导缓解治疗后。伊马替尼和尼洛替尼一般没有严重的感染并发症,但达沙替尼可能会略微增加机会性感染的风险。关于克唑替尼以及泛Trk抑制剂恩曲替尼和拉罗替尼的数据有限。使用替沙格韦单抗进行的嵌合抗原受体(CAR)T细胞疗法与儿童≥3级感染相关,并与HGG以及免疫相关不良事件的出现有关。奥英妥珠单抗、维布妥昔单抗和维奈克拉的非标签疗法显示与治疗相关的≥3级感染率较低,而在T细胞恶性肿瘤的标准化疗中添加硼替佐米似乎可以降低诱导期间的感染风险。本文还讨论了每种靶向药物的预防、免疫重建和疫苗接种,并与成人研究进行了比较。