Centre de Recherches Médicales de Lambaréné CERMEL, Hospital Albert Schweitzer, BP 242, Lambaréné, Gabon.
Center of Tropical Medicine and Travel Medicine, Department of Infectious Diseases, Amsterdam University Medical Centers, Location Amsterdam, Amsterdam Infection and Immunity, Amsterdam Public Health, University of Amsterdam, Meibergdreef 9, 1105 AZ, Amsterdam, The Netherlands.
Infection. 2023 Jun;51(3):697-704. doi: 10.1007/s15010-022-01941-5. Epub 2022 Oct 28.
Routinely generated surveillance data are important for monitoring the effectiveness of MDR-TB control strategies. Incidence of rifampicin-resistant tuberculosis (RR-TB) is a key indicator for monitoring MDR-TB.
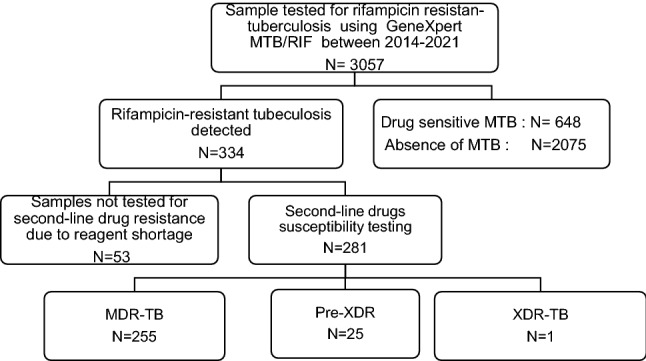
In a longitudinal nationwide retrospective study, 8 years (2014-2021) of sputum samples from presumptively drug-resistant tuberculosis patients from all regions of Gabon were referred to the national tuberculosis reference laboratory. Samples were analysed using GeneXpert MTB/RIF and Genotype MTBDRsl version 2/Line Probe Assay.
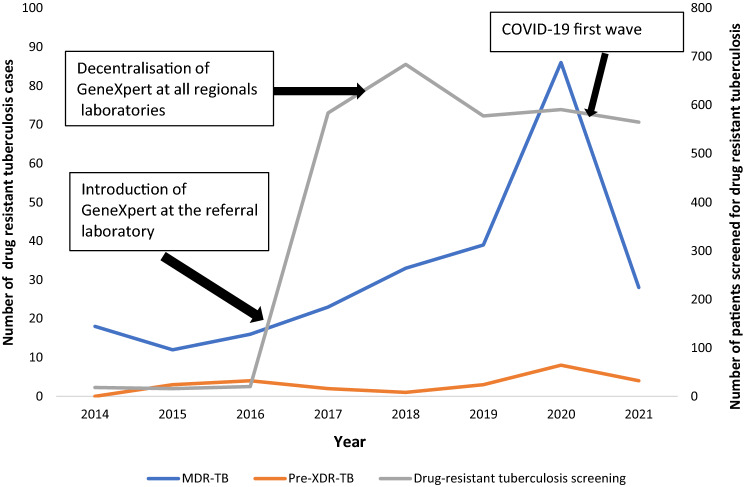
Of 3057 sputum samples from presumptive tuberculosis patients, both from local hospital and from referral patients, 334 were RR-TB. The median patient age was 33 years (interquartile range 26-43); one third was newly diagnosed drug-resistant tuberculosis patients; one-third was HIV-positive. The proportion of men with RR-TB was significantly higher than that of women (55% vs 45%; p < 0.0001). Patients aged 25-35 years were most affected (32%; 108/334). The cumulative incidence of RR-TB was 17 (95% CI 15-19)/100,000 population over 8 years. The highest incidences were observed in 2020 and 2021. A total of 281 samples were analysed for second-line drug resistance. The proportions of study participants with MDR-TB, pre-XDR-TB and XDR-TB were 90.7% (255/281), 9% (25/281) and 0.3% (1/281), respectively. The most-common mutations in fluoroquinolones resistance isolates was gyrA double mutation gyrA MUT3B and MUT3C (23%; 4/17). Most (64%; 6/8) second-line injectable drugs resistance isolates were characterised by missing both rrs WT2 and MUT2 banding.
The increasing incidence of MDR-TB infection in Gabon is alarming. It is highest in the 25-35 years age category. The incidence of MDR-TB infection in treatment-naïve patients calls for case finding and contact tracing strategy improvement.
常规生成的监测数据对于监测耐多药结核病(MDR-TB)控制策略的有效性非常重要。利福平耐药结核病(RR-TB)的发病率是监测 MDR-TB 的关键指标。
在一项全国性的纵向回顾性研究中,来自加蓬所有地区的疑似耐药结核病患者的 8 年(2014-2021 年)痰液样本被送到国家结核病参考实验室。使用 GeneXpert MTB/RIF 和 Genotype MTBDRsl 版本 2/Line Probe 检测法对样本进行分析。
在来自当地医院和转诊患者的 3057 份疑似肺结核患者的痰液样本中,有 334 份为 RR-TB。患者的中位年龄为 33 岁(四分位距 26-43 岁);三分之一为新诊断的耐药结核病患者;三分之一为 HIV 阳性。RR-TB 男性患者的比例明显高于女性(55%比 45%;p<0.0001)。25-35 岁的患者受影响最大(32%;108/334)。8 年内 RR-TB 的累积发病率为 17(95%CI 15-19)/100000 人。发病率最高的是 2020 年和 2021 年。共有 281 份样本进行二线药物耐药性分析。MDR-TB、预广泛耐药结核病(pre-XDR-TB)和广泛耐药结核病(XDR-TB)患者的比例分别为 90.7%(255/281)、9%(25/281)和 0.3%(1/281)。氟喹诺酮类耐药分离株中最常见的突变是 gyrA 双重突变 gyrA MUT3B 和 MUT3C(23%;4/17)。大多数(64%;6/8)二线注射用药物耐药分离株的特征是 rrs WT2 和 MUT2 带均缺失。
加蓬耐多药结核病感染的发病率不断上升令人担忧。发病率最高的是 25-35 岁年龄段。初治患者的 MDR-TB 感染发病率需要进行病例发现和接触者追踪策略的改进。