Kühl Melf-Jakob, Gondwe Thandile, Dhabangi Aggrey, Kwambai Titus K, Mori Amani T, Opoka Robert, John C Chandy, Idro Richard, Ter Kuile Feiko O, Phiri Kamija S, Robberstad Bjarne
Centre for International Health (CIH), Department of Global Public Health and Primary Care, University of Bergen, Årstadveien 17, 5009 Bergen, Norway.
Health Economics Leadership and Translational Ethics Research Group (HELTER), Department of Global Public Health and Primary Care, University of Bergen, Årstadveien 17, 5009 Bergen, Norway.
EClinicalMedicine. 2022 Oct 1;52:101669. doi: 10.1016/j.eclinm.2022.101669. eCollection 2022 Oct.
Children hospitalised with severe anaemia in malaria-endemic areas are at a high risk of dying or being readmitted within six months of discharge. A trial in Kenya and Uganda showed that three months of postdischarge malaria chemoprevention (PDMC) with monthly dihydroartemisinin-piperaquine (DP) substantially reduced this risk. The World Health Organization recently included PDMC in its malaria chemoprevention guidelines. We conducted a cost-effectiveness analysis of community-based PDMC delivery (supplying all three PDMC-DP courses to caregivers at discharge to administer at home), facility-based PDMC delivery (monthly dispensing of PDMC-DP at the hospital), and the standard of care (no PDMC).
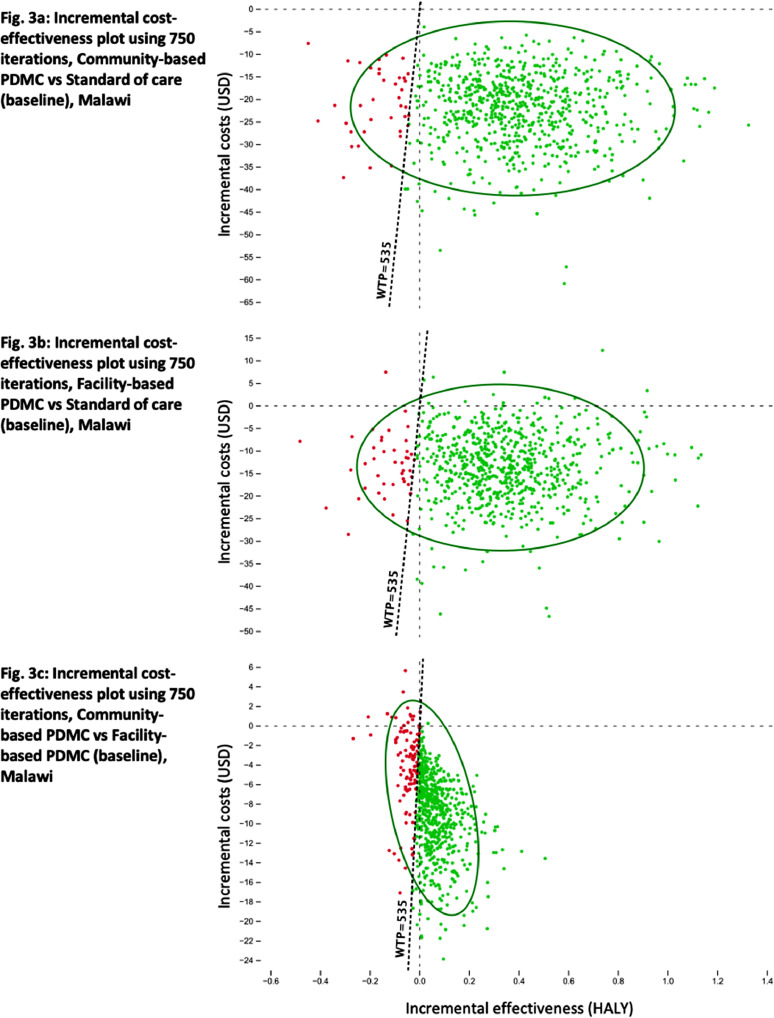
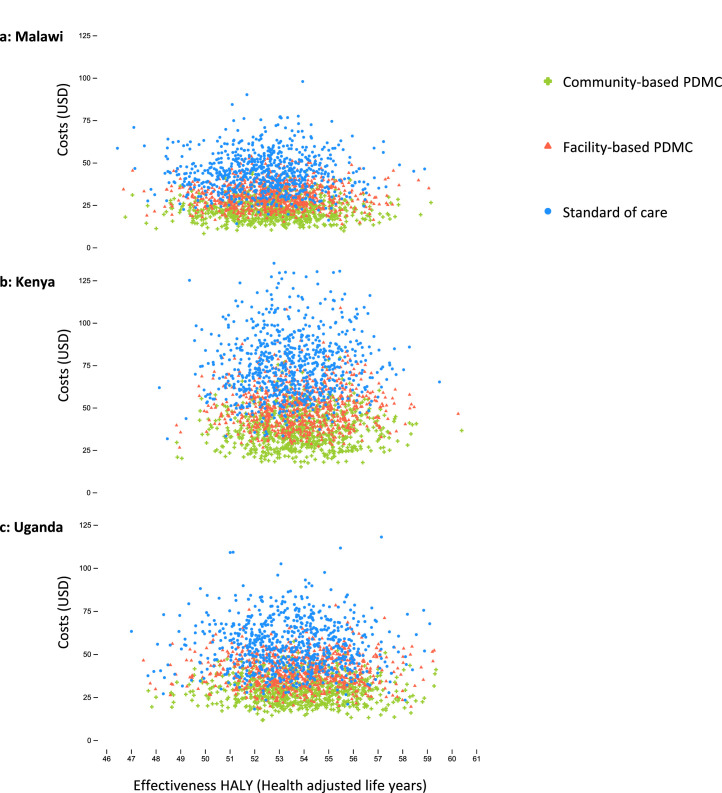
We combined data from two recently completed trials; one placebo-controlled trial in Kenya and Uganda collecting efficacy data (May 6, 2016 until November 15, 2018; n=1049), and one delivery mechanism trial from Malawi collecting adherence data (March 24, 2016 until October 3, 2018; n=375). Cost data were collected alongside both trials. Three Markov decision models, one each for Malawi, Kenya, and Uganda, were used to compute incremental cost-effectiveness ratios expressed as costs per quality-adjusted life-year (QALY) gained. Deterministic and probabilistic sensitivity analyses were performed to account for uncertainty.
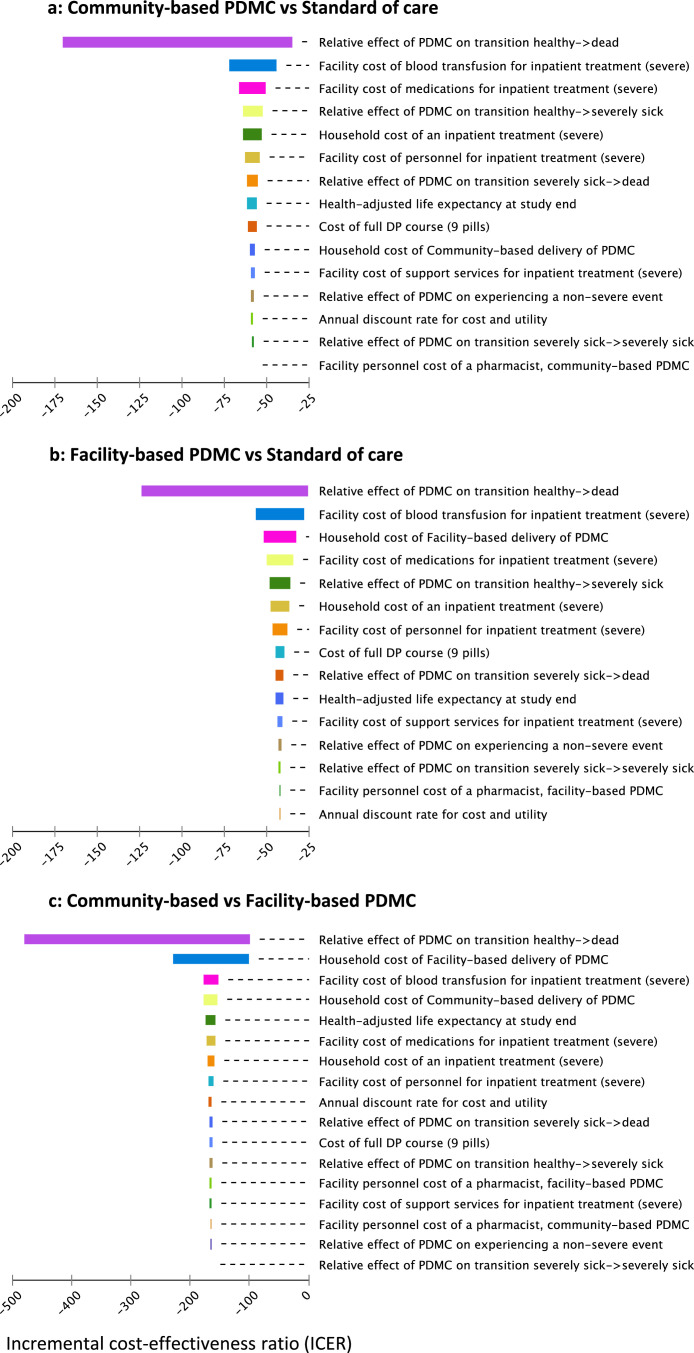
Both PDMC strategies were cost-saving in each country, meaning less costly and more effective in increasing health-adjusted life expectancy than the standard of care. The estimated incremental cost savings for community-based PDMC compared to the standard of care were US$ 22·10 (Malawi), 38·52 (Kenya), and 26·23 (Uganda) per child treated. The incremental effectiveness gain using either PDMC strategy varied between 0·3 and 0·4 QALYs. Community-based PDMC was less costly and more effective than facility-based PDMC. These results remained robust in sensitivity analyses.
PDMC under implementation conditions is cost-saving. Caregivers receiving PDMC at discharge is a cost-effective delivery strategy for implementation in malaria-endemic southeastern African settings.
Research Council of Norway.
在疟疾流行地区因严重贫血住院的儿童在出院后六个月内面临很高的死亡或再次入院风险。在肯尼亚和乌干达进行的一项试验表明,出院后三个月每月使用双氢青蒿素哌喹(DP)进行疟疾化学预防(PDMC)可大幅降低这种风险。世界卫生组织最近将PDMC纳入其疟疾化学预防指南。我们对基于社区的PDMC实施方式(在出院时向照顾者提供全部三个PDMC-DP疗程以便在家中给药)、基于医疗机构的PDMC实施方式(在医院每月分发PDMC-DP)以及标准治疗(不进行PDMC)进行了成本效益分析。
我们合并了两项最近完成的试验的数据;一项在肯尼亚和乌干达进行的安慰剂对照试验收集疗效数据(2016年5月6日至2018年11月15日;n = 1049),以及一项来自马拉维的实施方式试验收集依从性数据(2016年3月24日至2018年10月3日;n = 375)。两项试验同时收集成本数据。使用三个马尔可夫决策模型,分别针对马拉维、肯尼亚和乌干达,来计算以每获得一个质量调整生命年(QALY)的成本表示的增量成本效益比。进行确定性和概率敏感性分析以考虑不确定性。
在每个国家,两种PDMC策略均节省成本,这意味着与标准治疗相比,成本更低且在提高健康调整预期寿命方面更有效。与标准治疗相比,基于社区的PDMC每治疗一名儿童估计节省的增量成本分别为22.10美元(马拉维)、38.52美元(肯尼亚)和26.23美元(乌干达)。使用任何一种PDMC策略的增量效果增益在0.3至0.4个QALY之间。基于社区的PDMC比基于医疗机构的PDMC成本更低且更有效。这些结果在敏感性分析中仍然稳健。
在实施条件下,PDMC节省成本。让照顾者在出院时接受PDMC是在疟疾流行的非洲东南部地区实施的一种具有成本效益的实施策略。
挪威研究理事会。