Costa Laura, Martins José, Costa Marina, Oliveira Ana Isabel, Leal Dina, Lencastre Luís
Critical Care, Serviço de Medicina Intensiva, Hospital de Braga, Braga, PRT.
Internal Medicine, Hospital of Braga, Braga, PRT.
Cureus. 2022 Sep 26;14(9):e29610. doi: 10.7759/cureus.29610. eCollection 2022 Sep.
Severe COVID-19 is associated with serious complications and poor outcomes. Older age and underlying comorbidities are known risk factors for severe COVID-19, but a better understanding of baseline characteristics and outcomes of patients with severe COVID-19 is urgently needed.
This study was a retrospective case series of 227 consecutive patients with laboratory-confirmed COVID-19 admitted to the intensive care unit (ICU) at our institution between March 2020 and December 2021. Demographic and clinical data were collected.
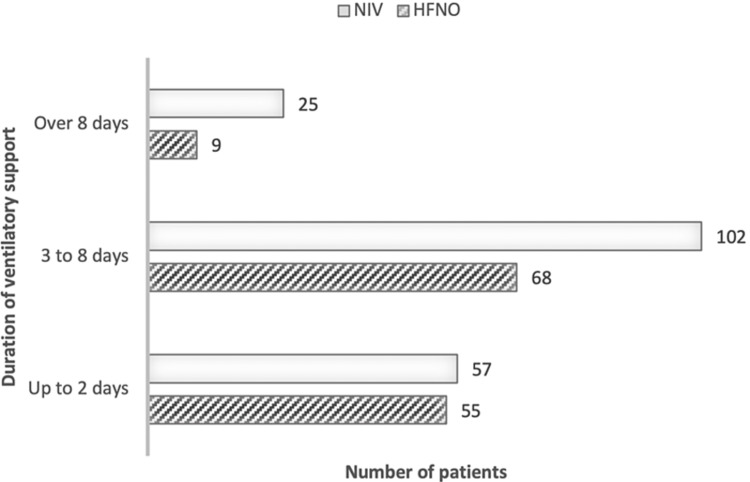
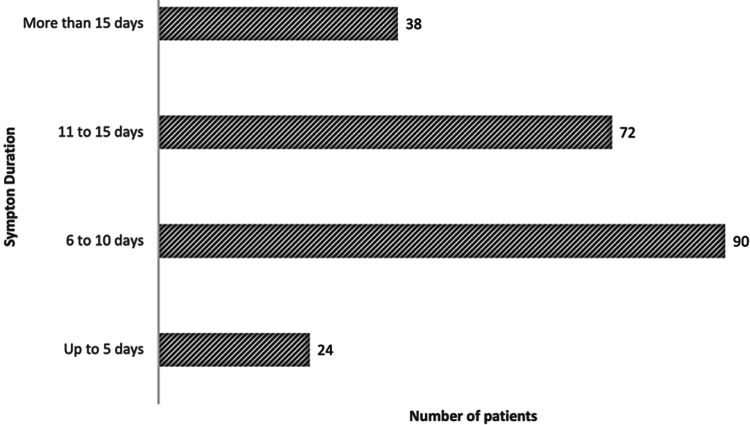
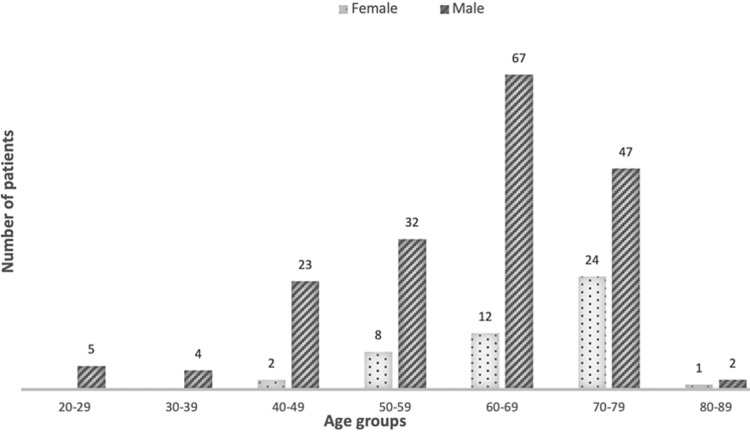
The median age of patients was 65 years, and 180 (79.3%) were male. Cardiovascular comorbidities were frequent and included hypertension (n=148; 65.2%), dyslipidemia (n=116; 51.1%), obesity (n=114; 50.2%), and diabetes mellitus (n=80; 35.2%). About 20% of the patients had the chronic respiratory disease, with sleep apnea being the most common. Immunosuppression was identified in 13% of the patients, with autoimmunity, post-transplantation, and neoplasms being the most represented causes. Most patients were admitted to the ICU at six to 15 days after symptom onset, corresponding to stages IIb (pulmonary involvement/hypoxia) and III (hyperinflammatory). All patients received systemic steroids, with an average treatment duration of 22 days. Several ventilatory support strategies were used; 80 patients were supported entirely noninvasively with high flow nasal oxygenation and noninvasive ventilation, while 164 patients were invasively ventilated. Most intubations (65%) occurred in the first 24 hours after admission, and the mean duration of mechanical ventilation was 14 days. The reintubation rate was 10%, occurring on average two to three days after planned extubation. Thirty-two tracheostomies were performed. Bacterial co-infection was treated in 75% of patients, and co-infection complicating COVID-19 pneumonia was diagnosed in eight patients. Median ICU and hospital stays were 15 and 25 days, respectively, and the 28-day mortality rate was 38%. Patients over 75 years experienced a higher mortality rate (56%). Increased age and multimorbidity, particularly comprising cardiovascular disease and associated risk factors, were significantly more common in patients who died within 28 days after ICU admission.
A large proportion of critically ill COVID-19 patients required prolonged mechanical ventilation. ICU/hospital stay and mortality were particularly elevated in older patients and patients with cardiovascular risk factors. Considerable discrepancy existed between the proportion of patients with microbiological documentation of bacterial infections and those receiving antimicrobials. Improved methods for adequate microbiological diagnosis are needed and stewardship programs should be reinforced.
重症新型冠状病毒肺炎(COVID-19)与严重并发症及不良预后相关。高龄和基础合并症是已知的重症COVID-19风险因素,但迫切需要更好地了解重症COVID-19患者的基线特征和预后。
本研究为回顾性病例系列研究,纳入了2020年3月至2021年12月期间在我院重症监护病房(ICU)连续收治的227例实验室确诊的COVID-19患者。收集了人口统计学和临床数据。
患者的中位年龄为65岁,男性180例(79.3%)。心血管合并症常见,包括高血压(n = 148;65.2%)、血脂异常(n = 116;51.1%)、肥胖(n = 114;50.2%)和糖尿病(n = 80;35.2%)。约20%的患者患有慢性呼吸系统疾病,其中睡眠呼吸暂停最为常见。13%的患者存在免疫抑制,自身免疫、移植后和肿瘤是最主要的原因。大多数患者在症状出现后6至15天入住ICU,对应IIb期(肺部受累/缺氧)和III期(高炎症期)。所有患者均接受全身糖皮质激素治疗,平均治疗时间为22天。采用了多种通气支持策略;80例患者完全通过高流量鼻导管给氧和无创通气进行无创支持,而164例患者接受有创通气。大多数插管(65%)发生在入院后的头24小时内,机械通气的平均持续时间为14天。再插管率为10%,平均发生在计划拔管后两到三天。实施了32例气管切开术。75%的患者接受了细菌合并感染的治疗,8例患者被诊断为COVID-19肺炎合并细菌感染。ICU和住院的中位时间分别为15天和25天,28天死亡率为38%。75岁以上患者的死亡率更高(56%)。年龄增加和多种合并症,特别是包括心血管疾病及相关风险因素,在ICU入院后28天内死亡的患者中明显更为常见。
很大一部分重症COVID-19患者需要长时间机械通气。老年患者和有心血管危险因素的患者的ICU/住院时间及死亡率尤其升高。有细菌感染微生物学记录的患者比例与接受抗菌药物治疗的患者比例之间存在相当大的差异。需要改进充分的微生物学诊断方法,并加强管理计划。