Department of Surgery, Emory University, Atlanta, Georgia, USA.
Department of Medicine, Emory University, Atlanta, Georgia, USA.
Transpl Infect Dis. 2022 Dec;24(6):e13983. doi: 10.1111/tid.13983. Epub 2022 Nov 14.
Belatacept improves long-term graft survival, but control of some primary viral infections may be impaired. We evaluated the impact of belatacept and tacrolimus on cytomegalovirus (CMV) viral control, remission and relapse in CMV high-risk and moderate-risk recipients.
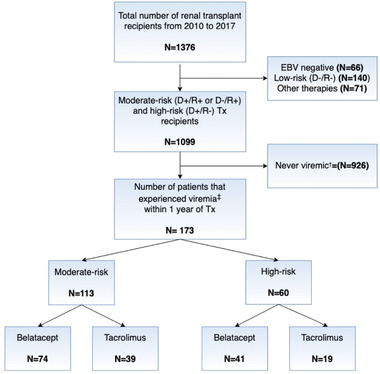
Using a multistate Markov model, we evaluated viral load state transitions of 173 kidney transplant recipients with at least one episode of viremia within 1 year after transplant: state 1, undetectable/low viral load; state 2, moderate viremia; and state 3, severe viremia.
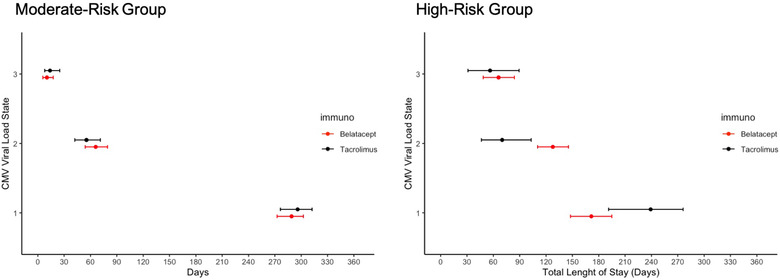
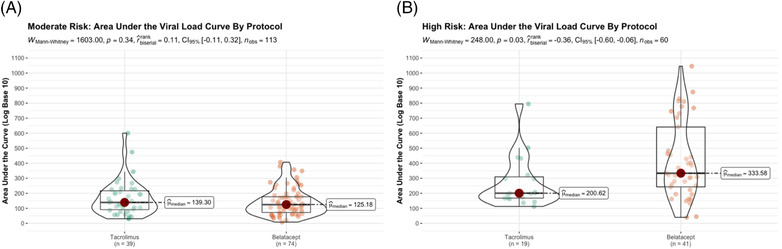
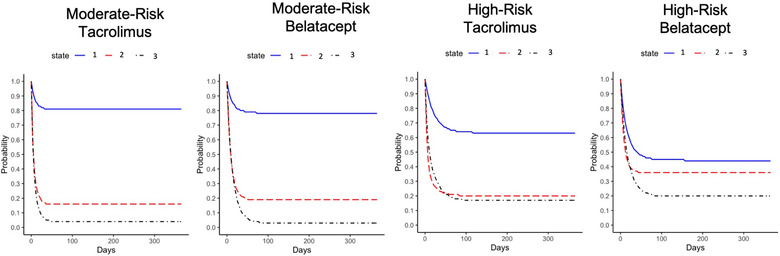
Among high-risk recipients, belatacept-treated recipients exhibited a significantly higher probability of entering moderate viremia (.36; 95% CI = .31, .41) than tacrolimus-treated recipients (.20; 95% CI = .13, .29). The expected number of days in viremic states differed. High-risk belatacept-treated recipients persisted in moderate viremia for significantly longer (128 days, 95% CI = 110, 146) than did tacrolimus-treated recipients (70.0 days, 95% CI = 45.2, 100) and showed a trend of shorter duration in low/undetectable viral load state (172 days, 95% CI = 148, 195) than did tacrolimus-treated recipients (239 days, 95% CI = 195, 277). Moderate-risk recipients showed better viral load control and with no differences by immunosuppression.
High-risk belatacept-treated recipients showed defects in sustaining viral control relative to tacrolimus-treated recipients. Avoidance of initial use belatacept in high-risk recipients or development of modified management protocols should be considered.
巴利昔单抗可改善长期移植物存活率,但某些原发性病毒感染的控制可能受损。我们评估了巴利昔单抗和他克莫司对巨细胞病毒(CMV)高危和中危受者病毒控制、缓解和复发的影响。
我们使用多状态马尔可夫模型,评估了 173 例移植后 1 年内至少有一次病毒血症发作的肾移植受者的病毒载量状态转变:状态 1,不可检测/低病毒载量;状态 2,中度病毒血症;状态 3,重度病毒血症。
在高危受者中,巴利昔单抗治疗组进入中度病毒血症的可能性显著高于他克莫司治疗组(0.36;95%CI=0.31,0.41)(0.20;95%CI=0.13,0.29)。处于病毒血症状态的预期天数不同。高危巴利昔单抗治疗组持续中度病毒血症的时间显著长于他克莫司治疗组(128 天,95%CI=110,146),且处于低/不可检测病毒载量状态的时间有缩短趋势(172 天,95%CI=148,195),短于他克莫司治疗组(239 天,95%CI=195,277)。中危受者显示出更好的病毒载量控制,且免疫抑制治疗无差异。
与他克莫司治疗组相比,高危巴利昔单抗治疗组在维持病毒控制方面存在缺陷。应考虑避免高危受者初始使用巴利昔单抗或制定改良的管理方案。