Department of Environmental Health, Harvard T. H. Chan School of Public Health, Massachusetts 02115, USA; Channing Division of Network Medicine, Department of Medicine, Brigham and Women's Hospital, Boston, MA 02115, USA.
Department of Environmental Health, Harvard T. H. Chan School of Public Health, Massachusetts 02115, USA; Channing Division of Network Medicine, Department of Medicine, Brigham and Women's Hospital, Boston, MA 02115, USA; Department of Epidemiology, Harvard T. H. Chan School of Public Health, Boston, MA 02115, USA.
Environ Res. 2023 Jan 1;216(Pt 3):114684. doi: 10.1016/j.envres.2022.114684. Epub 2022 Nov 2.
Short-term exposure to high or low temperatures is associated with increased mortality and morbidity. Less is known about effects of long-term exposure to high or low temperatures. Prolonged exposure to high or low temperatures might contribute to pathophysiological mechanisms, thereby influencing the development of diseases. Our aim was to evaluate associations of long-term temperature exposure with cardiovascular disease (CVD) hospitalizations.
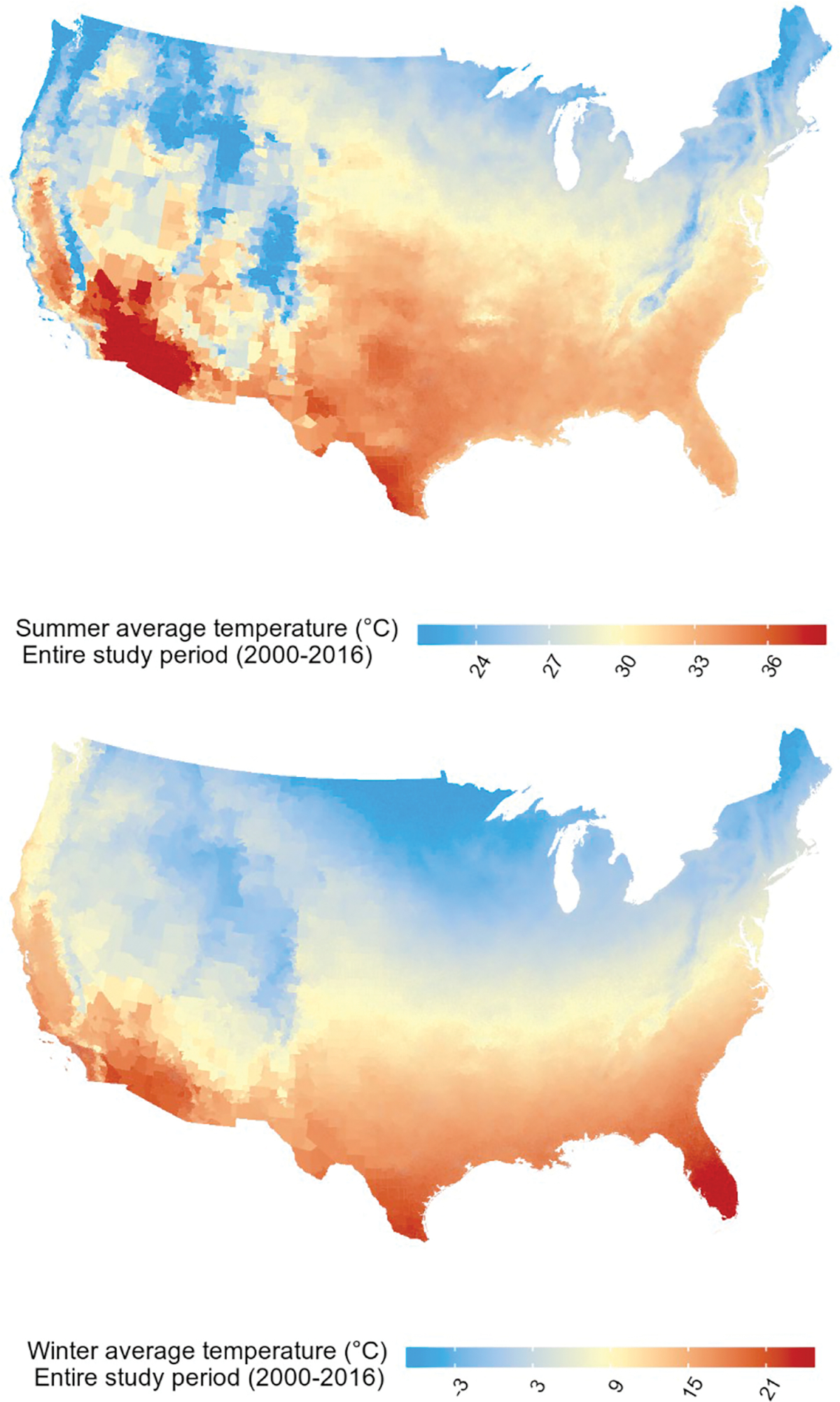
We constructed an open cohort consisting of all fee-for-service Medicare beneficiaries, aged ≥65, living in the contiguous US from 2000 through 2016 (∼61.6 million individuals). We used data from the 4 km Gridded Surface Meteorological dataset to assess the summer (June-August) and winter (December-February) average daily maximum temperature for each year for each zip code. Cox-equivalent Poisson models were used to estimate associations with first CVD hospitalization, after adjustment for potential confounders. We performed stratified analyses to assess potential effect modification by sex, age, race, Medicaid eligibility and relative humidity.
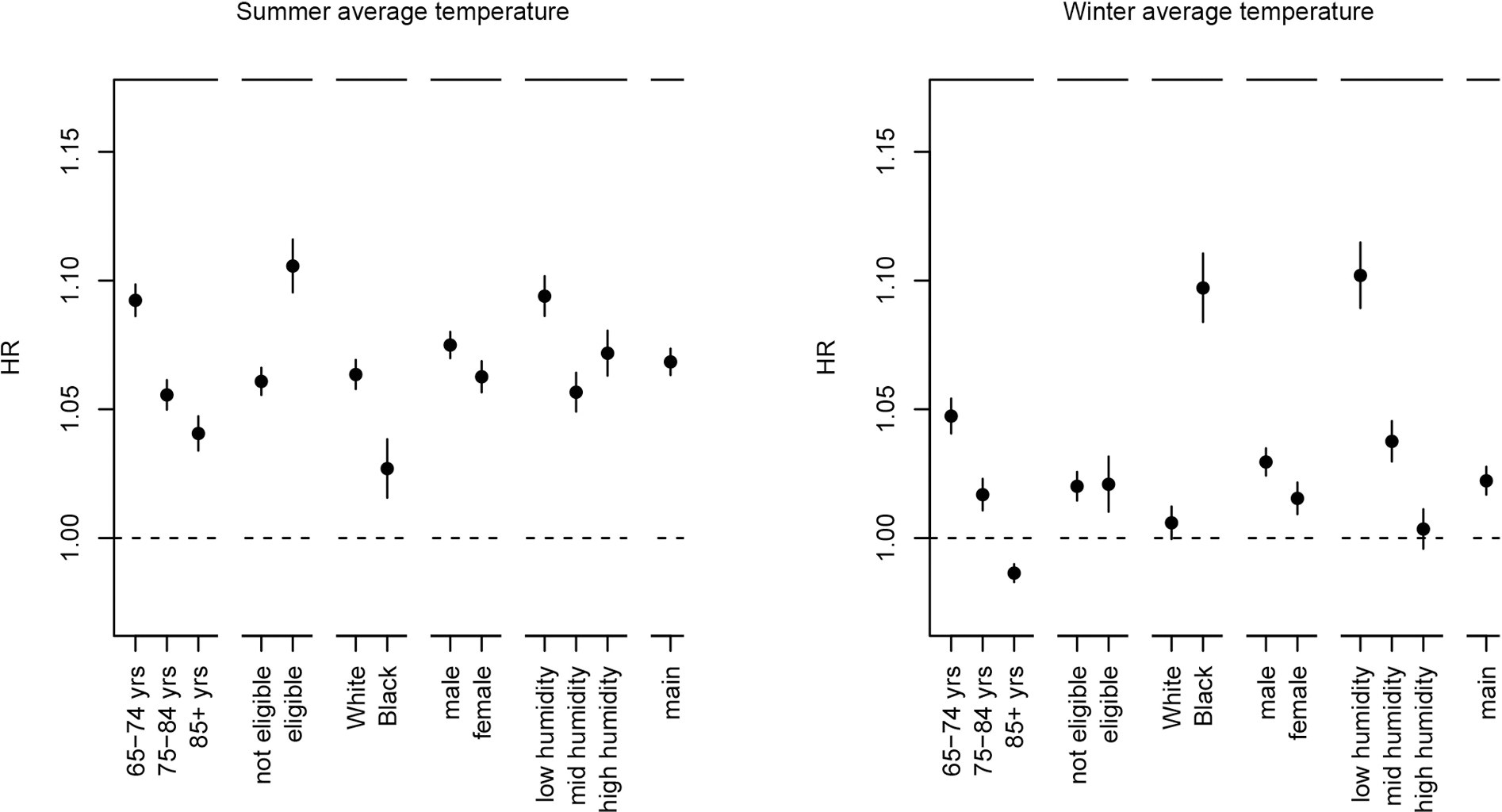
Higher summer average and lower winter average temperatures were associated with an increased risk of CVD hospitalization. We found a HR of 1.068 (95% CI: 1.063, 1.074) per IQR increase (5.2 °C) for summer average temperature and a HR of 1.022 (95% CI: 1.017, 1.028) per IQR decrease (11.7 °C) for winter average temperature. Positive associations of higher summer average temperatures were strongest for individuals aged <75 years, Medicaid eligible, and White individuals. Positive associations of lower winter average temperatures were strongest for individuals aged <75 years and Black individuals, and individuals living in low relative humidity areas.
Living in areas with high summer average temperatures or low winter average temperatures could increase the risk of CVD hospitalizations. The magnitude of the associations of summer and winter average temperatures differs by demographics and relative humidity levels.
短期暴露于高温或低温会增加死亡率和发病率。对于长期暴露于高温或低温的影响知之甚少。长时间暴露于高温或低温可能会导致病理生理机制,从而影响疾病的发展。我们的目的是评估长期温度暴露与心血管疾病(CVD)住院之间的关系。
我们构建了一个开放队列,该队列由 2000 年至 2016 年期间居住在美国大陆的所有有费用支付的医疗保险受益人(年龄≥65 岁,约 6160 万人)组成。我们使用 4km 网格化表面气象数据集的数据来评估每个邮政编码每年夏季(6 月至 8 月)和冬季(12 月至 2 月)的平均日最高温度。使用 Cox 等效泊松模型,在调整潜在混杂因素后,评估与首次 CVD 住院的关联。我们进行了分层分析,以评估性别、年龄、种族、医疗补助资格和相对湿度的潜在效应修饰作用。
夏季平均温度升高和冬季平均温度降低与 CVD 住院风险增加有关。我们发现,夏季平均温度每升高一个 IQR(5.2°C),风险比(HR)为 1.068(95%CI:1.063,1.074),冬季平均温度每降低一个 IQR(11.7°C),HR 为 1.022(95%CI:1.017,1.028)。对于年龄<75 岁、有医疗补助资格和白人的个体,较高的夏季平均温度的正相关关系最强。对于年龄<75 岁和黑人的个体,以及居住在相对湿度较低地区的个体,较低的冬季平均温度的正相关关系最强。
生活在夏季平均温度较高或冬季平均温度较低的地区可能会增加 CVD 住院的风险。夏季和冬季平均温度与人口统计学和相对湿度水平的关联程度不同。