Department of Medicine, University of California, Los Angeles, David Geffen School of Medicine, Los Angeles, California, USA.
Department of Pathology and Laboratory Medicine, Hospital of the University of Pennsylvania, Philadelphia, Pennsylvania, USA.
Cancer. 2023 Jan 1;129(1):89-97. doi: 10.1002/cncr.34490. Epub 2022 Nov 7.
Evidence exists that escalating melanoma incidence is due in part to overdiagnosis, the diagnosis of lesions that will not lead to symptoms or death. The authors aimed to characterize subsets of melanoma patients with very-low risk of death that may be contributing to overdiagnosis.
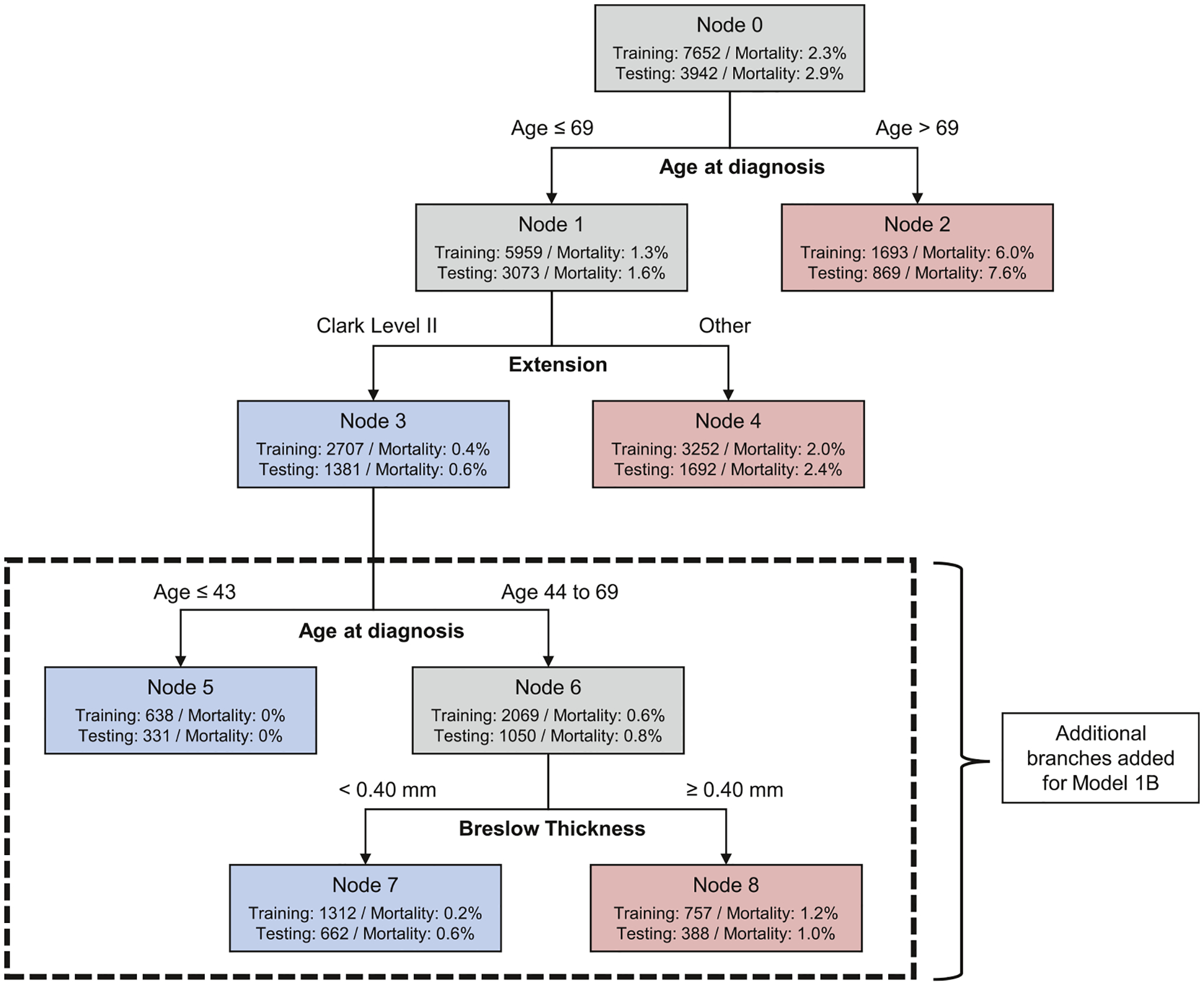
Melanoma patients diagnosed in 2010 and 2011 with stage I lesions ≤1.0 mm thick and negative clinical lymph nodes from the Surveillance, Epidemiology, and End Results database were selected. Classification and regression tree and logistic regression models were developed and validated to identify patients with very-low risk of death from melanoma within 7 years. Logistic models were also used to identify patients at higher risk of death among this group of stage I patients.
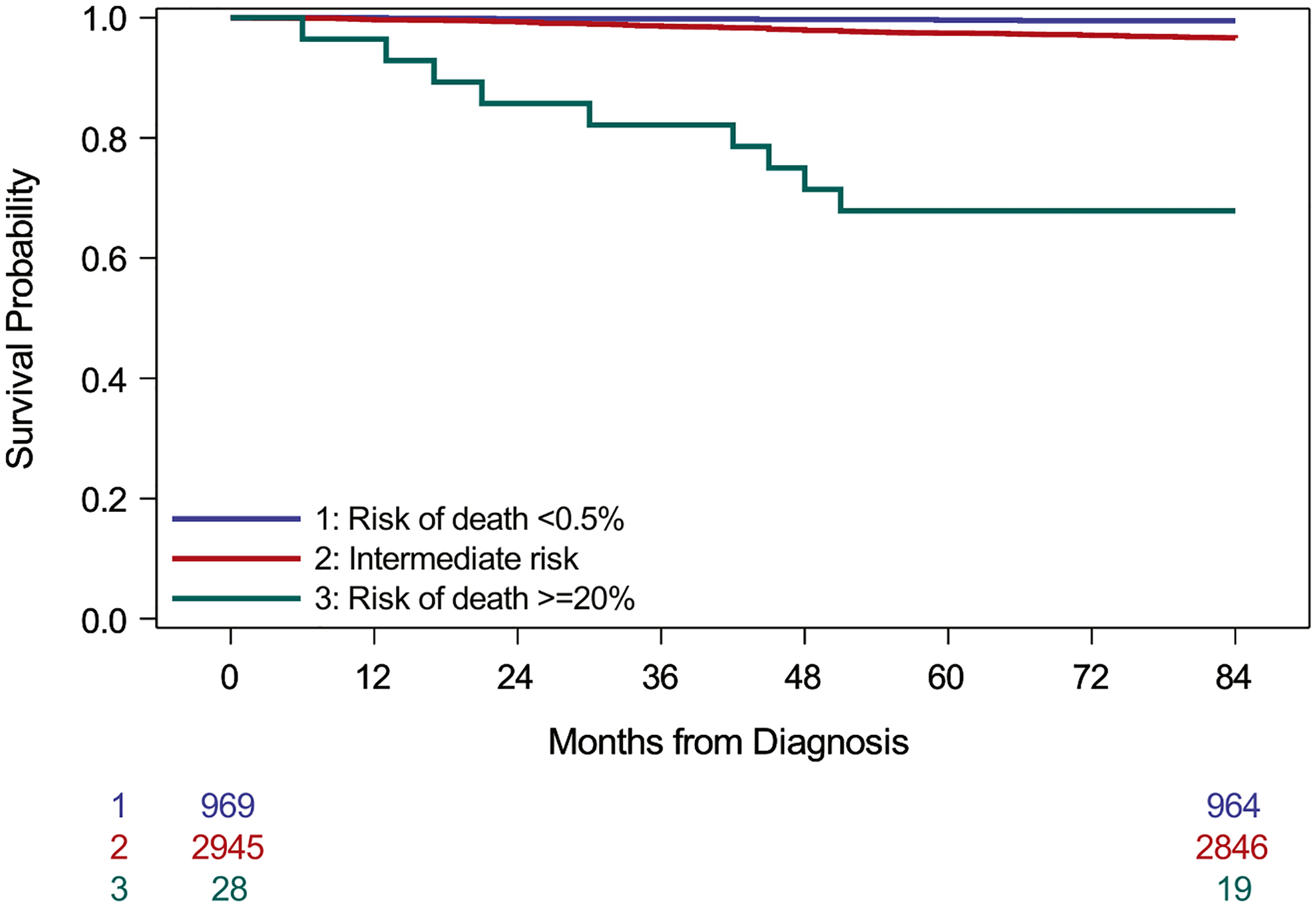
Compared to an overall 7-year mortality from melanoma of 2.5% in these patients, a subset comprising 25% had a risk below 1%. Younger age at diagnosis and Clark level II were associated with low risk of death in all models. Breslow thickness below 0.4 mm, absence of mitogenicity, absence of ulceration, and female sex were also associated with lower mortality. A small subset of high-risk patients with >20% risk of death was also identified.
Patients with very-low risk of dying from melanoma within 7 years of diagnosis were identified. Such cases warrant further study and consensus discussion to develop classification criteria, with the potential to be categorized using an alternative term such as "melanocytic neoplasms of low malignant potential."
Although melanoma is the most serious skin cancer, most melanoma patients have high chances of survival. There is evidence that some lesions diagnosed as melanoma would never have caused symptoms or death, a phenomenon known as overdiagnosis. In this study, we used cancer registry data to identify a subset of early-stage melanoma patients with almost no melanoma deaths. Using two statistical approaches, we identified patients with <1% risk of dying from melanoma in 7 years. Such patients tended to be younger with minimal invasion into the skin. We also identified a very small patient subset with higher mortality risk.
有证据表明,黑色素瘤发病率的上升部分归因于过度诊断,即诊断出不会导致症状或死亡的病变。作者旨在描述具有极低死亡风险的黑色素瘤患者亚组,这些患者可能导致过度诊断。
从监测、流行病学和最终结果数据库中选择 2010 年和 2011 年诊断为 I 期病变厚度≤1.0 毫米且临床淋巴结阴性的黑色素瘤患者。建立并验证分类回归树和逻辑回归模型,以确定 7 年内黑色素瘤死亡风险极低的患者。逻辑模型也用于识别该组 I 期患者中死亡风险较高的患者。
与这些患者 7 年黑色素瘤总体死亡率 2.5%相比,一个由 25%患者组成的亚组的风险低于 1%。所有模型中,诊断时年龄较小和 Clark 分级 II 与较低的死亡风险相关。Breslow 厚度<0.4 毫米、无有丝分裂活性、无溃疡和女性也与较低的死亡率相关。还确定了一小部分死亡风险>20%的高危患者。
确定了 7 年内死于黑色素瘤风险极低的患者。这些病例值得进一步研究和共识讨论,以制定分类标准,并有可能使用替代术语(如“低恶性潜能的黑素细胞瘤”)进行分类。
虽然黑色素瘤是最严重的皮肤癌,但大多数黑色素瘤患者有很高的生存机会。有证据表明,一些被诊断为黑色素瘤的病变永远不会引起症状或死亡,这种现象被称为过度诊断。在这项研究中,我们使用癌症登记数据来识别一组早期黑色素瘤患者,他们几乎没有黑色素瘤死亡。使用两种统计方法,我们确定了在 7 年内死于黑色素瘤风险<1%的患者。这些患者往往更年轻,皮肤侵犯程度更低。我们还确定了一个死亡率风险较高的非常小的患者亚组。