De Rosa Andrea, Di Somma Alberto, Mosteiro Alejandra, Ferrés Abel, Reyes Luis Alberto, Roldan Pedro, Torné Ramon, Torales Jorge, Solari Domenico, Cavallo Luigi Maria, Enseñat Joaquim, Prats-Galino Alberto
Division of Neurosurgery, Department of Neurosciences, Reproductive and Odontostomatological Sciences, Università degli Studi di Napoli "Federico II", Naples, Italy.
Department of Neurosurgery, Hospital Clinic, Barcelona, Spain.
Front Surg. 2022 Oct 21;9:1007447. doi: 10.3389/fsurg.2022.1007447. eCollection 2022.
Superior eyelid endoscopic transorbital approach (SETOA) is nowadays gaining progressive application in neurosurgical scenarios. Both anatomic and clinical reports have demonstrated the possibility of taking advantage of the orbital corridor as a minimally invasive route to reach anterior and middle cranial fossae and manage selected surgical lesions developing in these areas. The aim of this paper is to further shed light on other anatomic regions of the skull base as seen from a transorbital perspective, namely, the posterior cranial fossa and tentorial area, describing technical feasibility and steps in reaching this area through an extradural-transtentorial approach and providing quantitative evaluations of the "working area" obtained through this route.
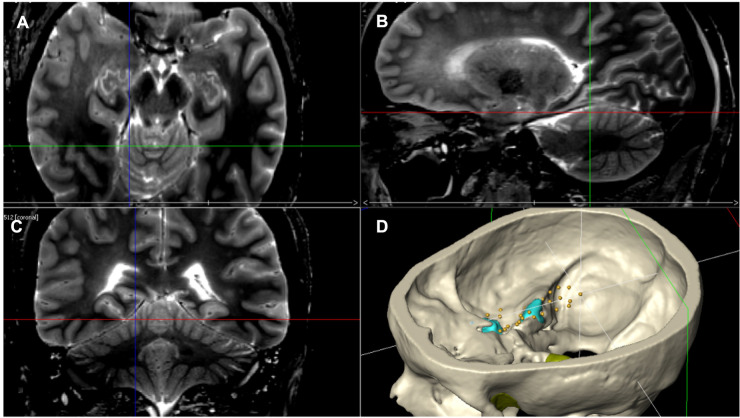
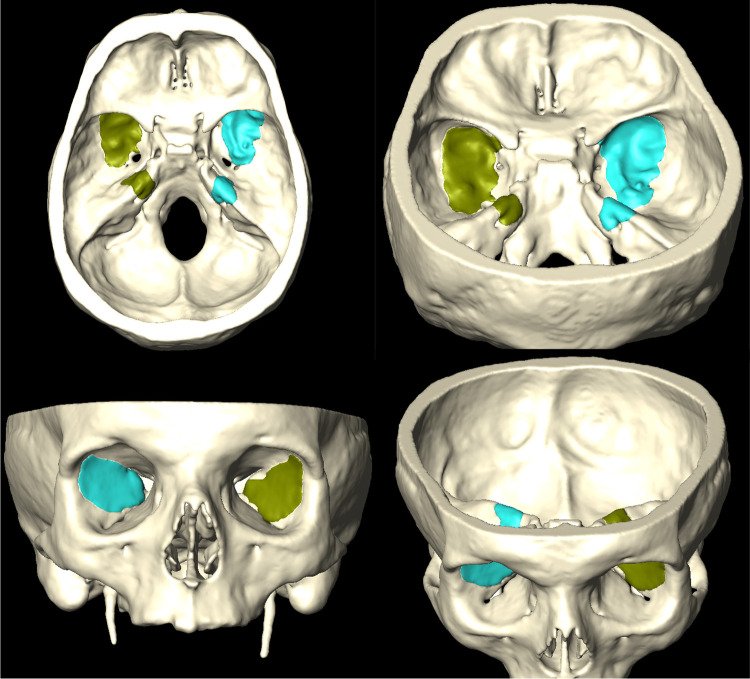
Four cadaveric heads (eight sides) were dissected at the Laboratory of Surgical Neuroanatomy (LSNA) of the University of Barcelona, Spain. A stepwise dissection of the transorbital approach to the tentorial area was described. Qualitative anatomical descriptions and quantitative analyses of working were evaluated by using pre- and postdissections CT and MRI scans, and three-dimensional reconstructions were made using Amira software.
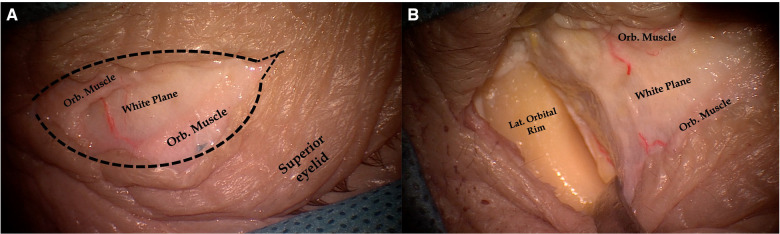
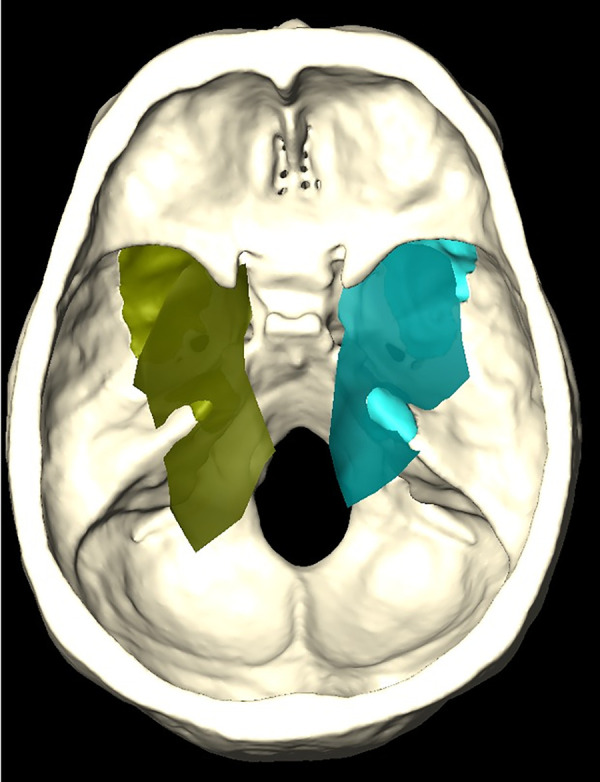
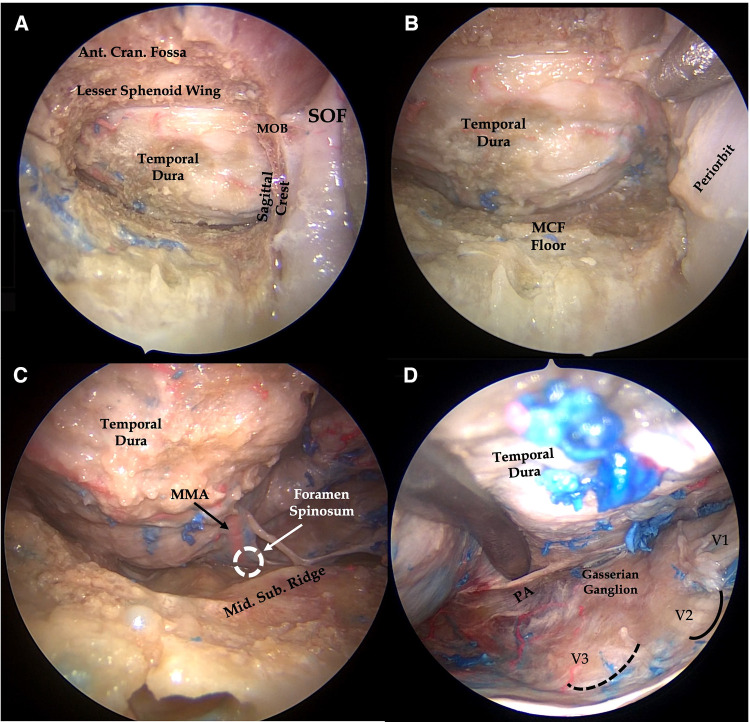
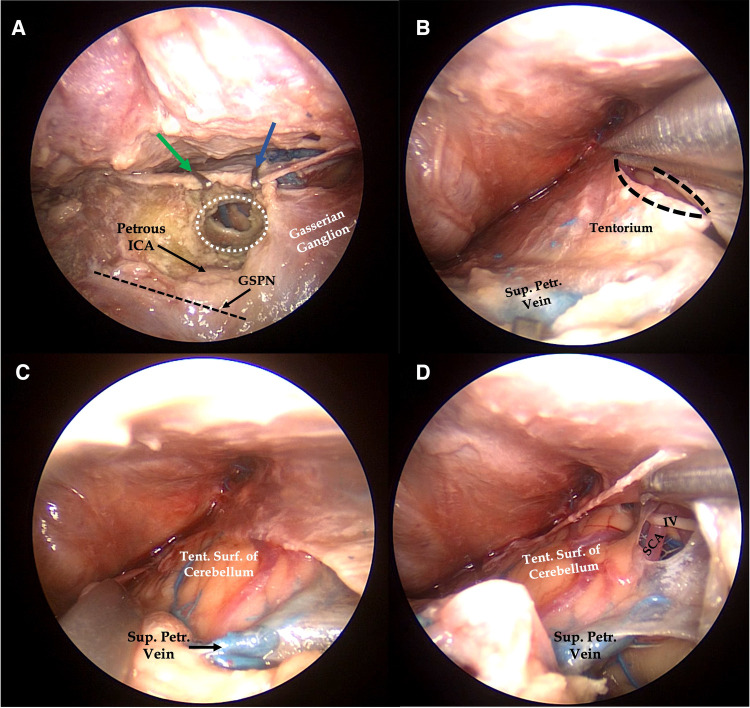
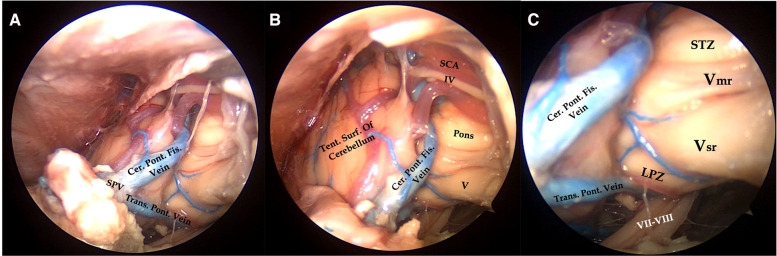
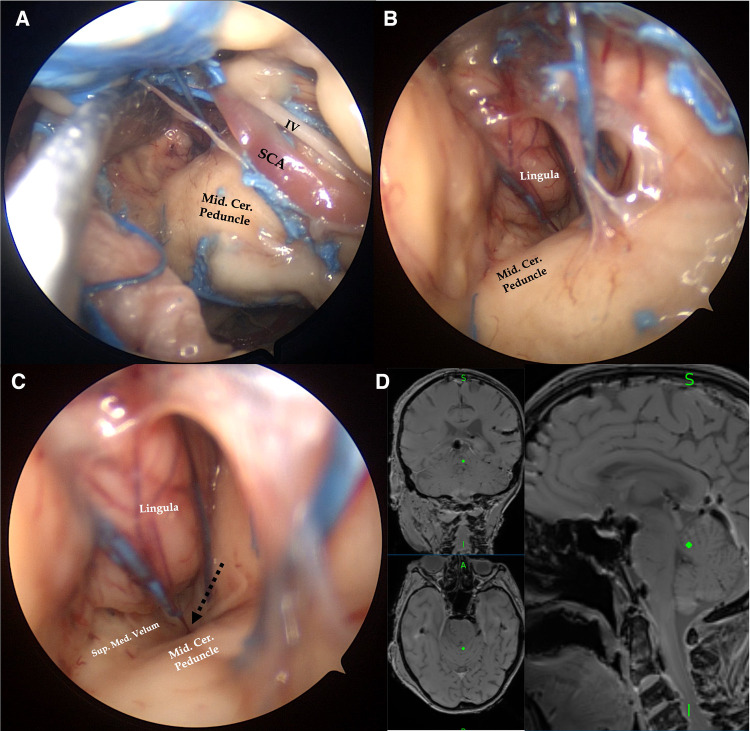
With the endoscopic transorbital approach, posterior cranial fossa dura was reached by an extradural middle cranial fossa approach and drilling of the petrous apex. After clipping the superior petrosal sinus, the tentorium was divided and cut. An endoscope was then introduced in the posterior cranial fossa at the level of the tentorial incisura. Qualitative analysis provided a description of the tentorial and petrosal surfaces of the cerebellum, middle tentorial incisura, cerebellopontine fissures, and, after arachnoid dissection, by a 30° endoscopic visualization, the posterior aspect of the cerebellomesencephalic fissure. Quantitative analysis of the "working area" obtained after bone removal was also provided.
This anatomic qualitative and quantitative study sheds light on the anatomy of the posterior cranial fossa contents, such as the tentorial area and incisura, as seen through a transorbital perspective. The first aim of the article is to enrich the anatomical knowledge as seen through this relatively new corridor and to provide quantitative details and insights into the technical feasibility of reaching these regions in a surgical scenario.
上睑内镜经眶入路(SETOA)如今在神经外科手术中得到越来越广泛的应用。解剖学和临床报告均已证实,利用眶部通道作为微创路径到达前颅窝和中颅窝并处理这些区域发生的特定手术病变是可行的。本文旨在从经眶视角进一步阐明颅底的其他解剖区域,即后颅窝和小脑幕区域,描述通过硬膜外 - 经小脑幕入路到达该区域的技术可行性和步骤,并对通过该路径获得的“工作区域”进行定量评估。
在西班牙巴塞罗那大学的外科神经解剖学实验室(LSNA)对4具尸体头部(8侧)进行解剖。描述了经眶入路至小脑幕区域的逐步解剖过程。通过解剖前和解剖后的CT及MRI扫描对工作的定性解剖描述和定量分析进行评估,并使用Amira软件进行三维重建。
采用内镜经眶入路,通过硬膜外中颅窝入路和磨除岩尖到达后颅窝硬脑膜。夹闭岩上窦后,切开并切断小脑幕。然后将内镜经小脑幕切迹置入后颅窝。定性分析描述了小脑幕和小脑岩面、小脑幕切迹中部、小脑脑桥裂,蛛网膜切开后,通过30°内镜观察,还描述了小脑脑桥裂的后部。还提供了去除骨质后获得的“工作区域”的定量分析。
这项解剖学定性和定量研究从经眶视角阐明了后颅窝内容物的解剖结构,如小脑幕区域和切迹。本文的首要目的是丰富通过这一相对较新的通道所观察到的解剖学知识,并提供定量细节以及对手术中到达这些区域的技术可行性的见解。