Department of Urology, Zhongda Hospital, Southeast University, Nanjing, China.
Institute of Urology, Medical School, Southeast University, Nanjing, China.
Ren Fail. 2022 Dec;44(1):1938-1947. doi: 10.1080/0886022X.2022.2142138.
Coagulation factors participates in the inflammatory cascade, known to play a crucial role in the development of acute kidney injury (AKI). Thus, it's likely that some factors may be associated with AKI. Among them, low levels of fibrinogen and antithrombin III (ATIII) activity have been proved to increase mortality in patients with sepsis. Moreover, they are also reported to be associated with higher incidence of AKI. However, the association between coagulation parameters, especially fibrinogen and ATIII, and prognosis of AKI has not been examined.
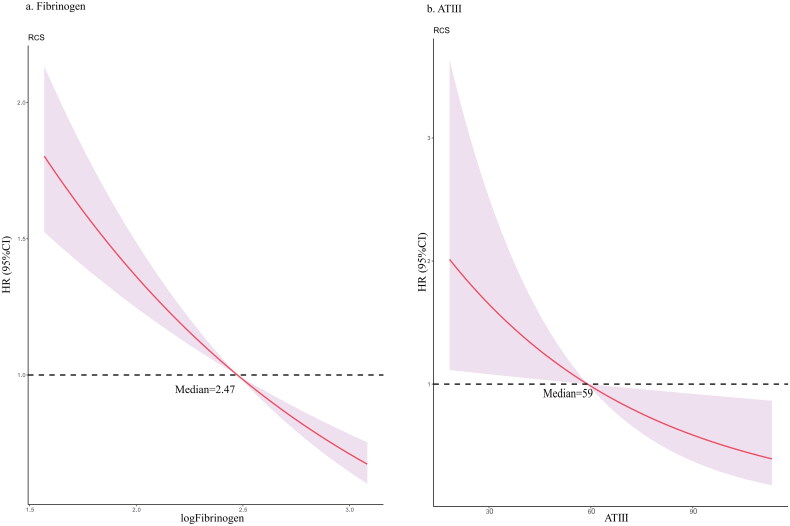
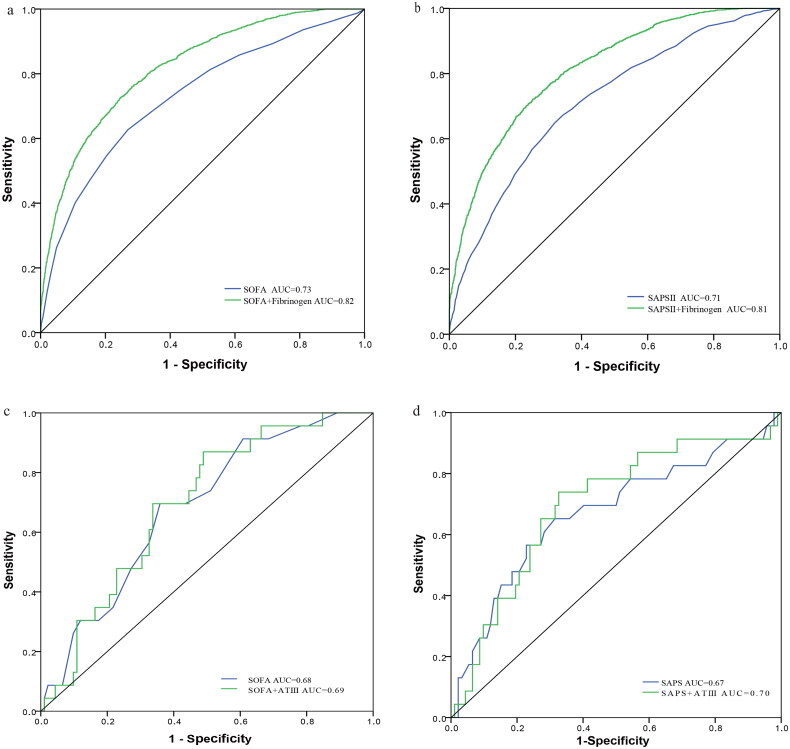
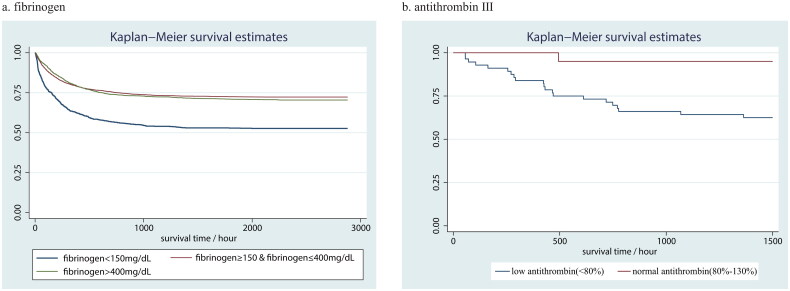
Data were acquired from Multiparameter Intelligent Monitoring in Intensive Care Database IV (MIMIC-IV) version 1.0. Cox proportional hazards regression model was used to estimate the relationship between coagulation parameters and in-hospital mortality in critically ill patients with AKI. Subgroup analysis was also conducted to assess the robustness of the association. Restricted cubic spline (RCS) curve was utilized to examine the nonlinear relationships between fibrinogen or ATIII and in-hospital mortality. Kaplan-Meier method was used to estimate cumulative incidence of mortality by fibrinogen or ATIII levels. Receiver-operating characteristic (ROC) curve was plotted and area under curve was calculated to evaluate predictive ability of fibrinogen or ATIII.
A total of 5914 eligible patients were enrolled in fibrinogen cohort study and 115 patients were eligible for ATIII cohort study. The baseline of low fibrinogen (<150 mg/dL) or ATIII (<80%) activity was associated with significantly higher in-hospital mortality (fibrinogen HR [95% CIs] 2.01 [1.79, 2.27]; ATIII 3.73 [1.11, 12.54]). The HR [95% CIs] of low fibrinogen remained significant 1.29 (1.13, 1.48) in multivariate analysis. The RCS curve showed nearly linear relationship. Subgroup analysis also proved the robustness of the association between fibrinogen and in-hospital mortality. Kaplan-Meier survival curve and ROC demonstrated the predictive capability of fibrinogen and ATIII.
Low fibrinogen is an independent predictor of in-hospital mortality in critically ill patients with AKI. Low ATIII activity is also likely to impact the risk of in-hospital death.
凝血因子参与炎症级联反应,在急性肾损伤(AKI)的发生发展中起着至关重要的作用。因此,某些因素可能与 AKI 相关。其中,纤维蛋白原和抗凝血酶 III(ATIII)活性降低已被证明会增加脓毒症患者的死亡率。此外,它们也与 AKI 的发生率升高有关。然而,凝血参数,特别是纤维蛋白原和 ATIII,与 AKI 预后之间的关系尚未得到检验。
数据来自多参数智能监护的重症监护数据库 IV(MIMIC-IV)版本 1.0。使用 Cox 比例风险回归模型来估计 AKI 危重症患者凝血参数与院内死亡率之间的关系。还进行了亚组分析以评估关联的稳健性。限制性立方样条(RCS)曲线用于检查纤维蛋白原或 ATIII 与院内死亡率之间的非线性关系。Kaplan-Meier 法用于根据纤维蛋白原或 ATIII 水平估计死亡率的累积发生率。绘制受试者工作特征(ROC)曲线并计算曲线下面积以评估纤维蛋白原或 ATIII 的预测能力。
共纳入 5914 例符合条件的患者进行纤维蛋白原队列研究,115 例符合 ATIII 队列研究条件。低纤维蛋白原(<150mg/dL)或 ATIII(<80%)活性的基线与院内死亡率显著升高相关(纤维蛋白原 HR [95%CI] 2.01 [1.79, 2.27];ATIII 3.73 [1.11, 12.54])。多变量分析中,低纤维蛋白原的 HR [95%CI] 仍有显著意义 1.29(1.13, 1.48)。RCS 曲线显示几乎呈线性关系。亚组分析也证明了纤维蛋白原与院内死亡率之间关联的稳健性。Kaplan-Meier 生存曲线和 ROC 表明了纤维蛋白原和 ATIII 的预测能力。
低纤维蛋白原是 AKI 危重症患者院内死亡率的独立预测因子。ATIII 活性降低也可能影响院内死亡风险。