Chronic Pain Research Group, Division of Population Health and Genomics, Mackenzie Building, Ninewells Hospital and Medical School, University of Dundee, Kirsty Semple Way, Dundee, DD2 4BF, UK.
Pat Macpherson Centre for Pharmacogenetics and Pharmacogenomics, Division of Population Health and Genomics, Ninewells Hospital and Medical School, University of Dundee, Dundee, UK.
J Neurol. 2023 Feb;270(2):1076-1094. doi: 10.1007/s00415-022-11478-0. Epub 2022 Nov 10.
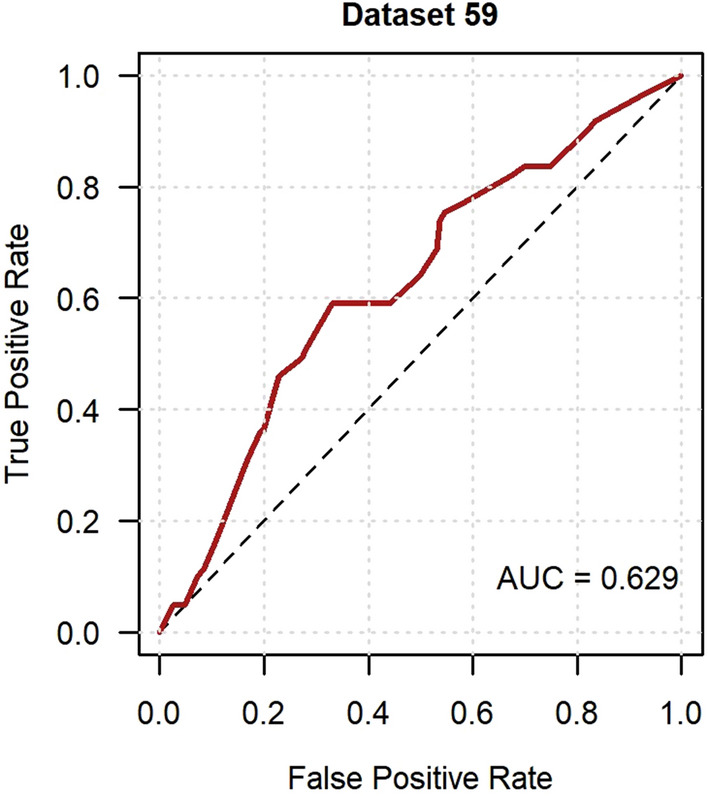
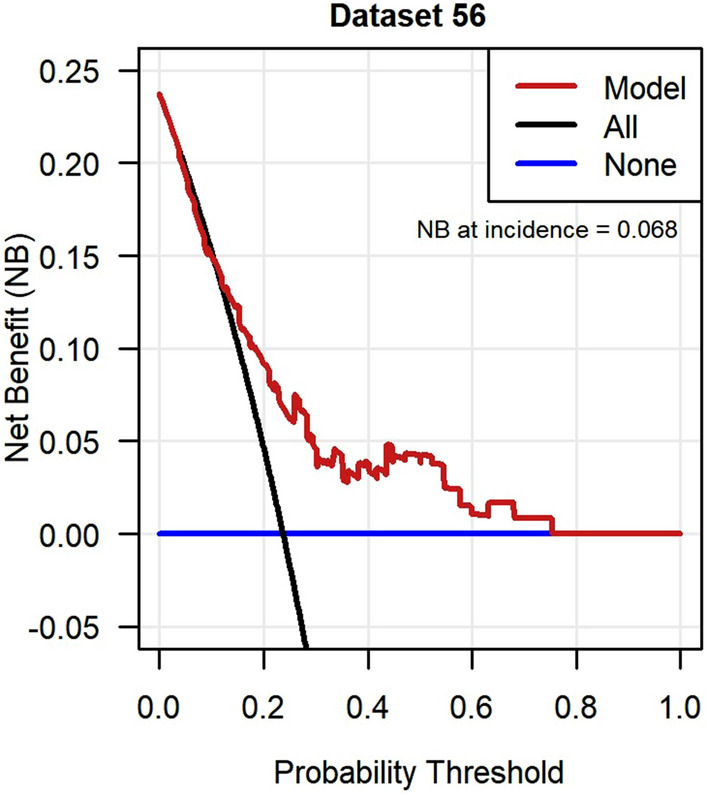
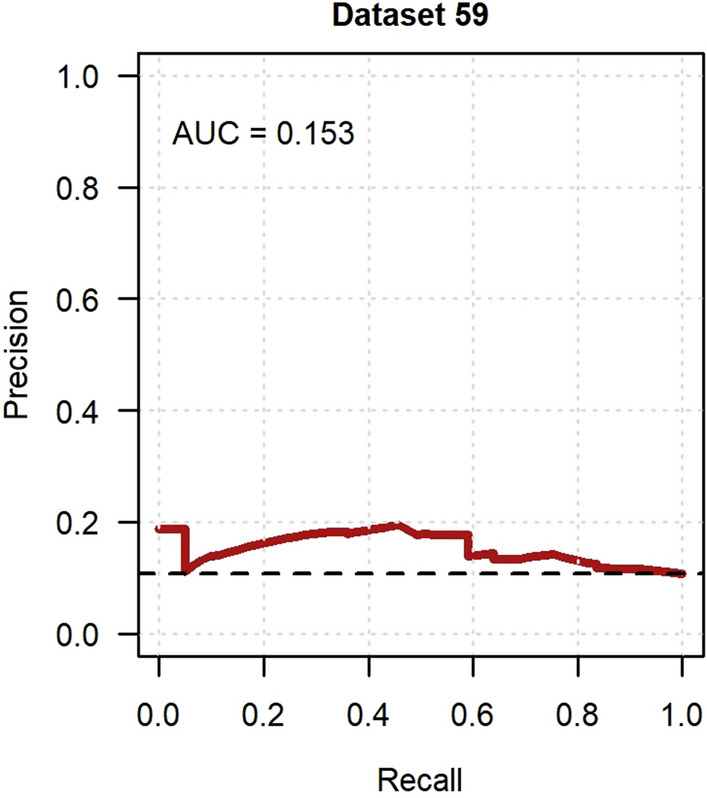
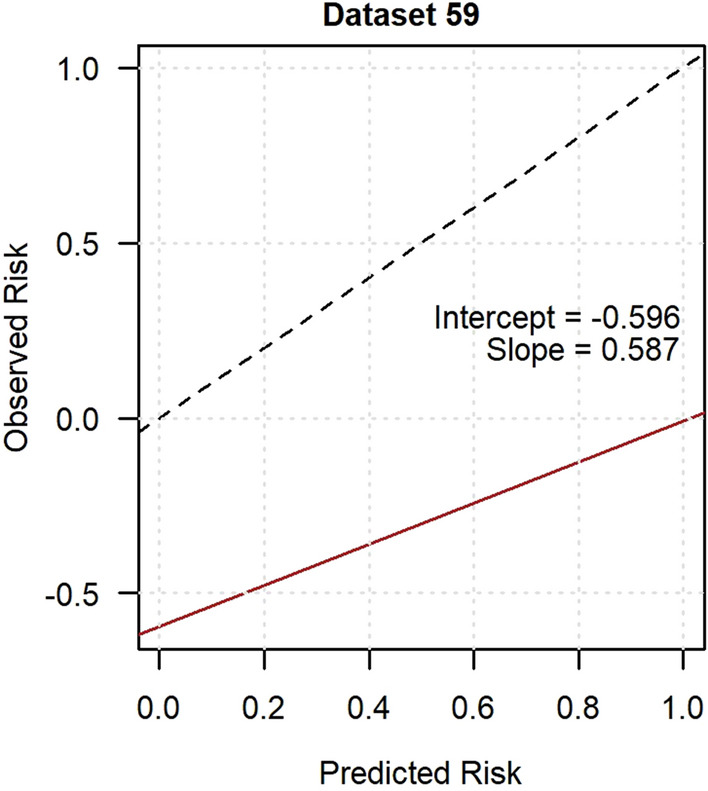
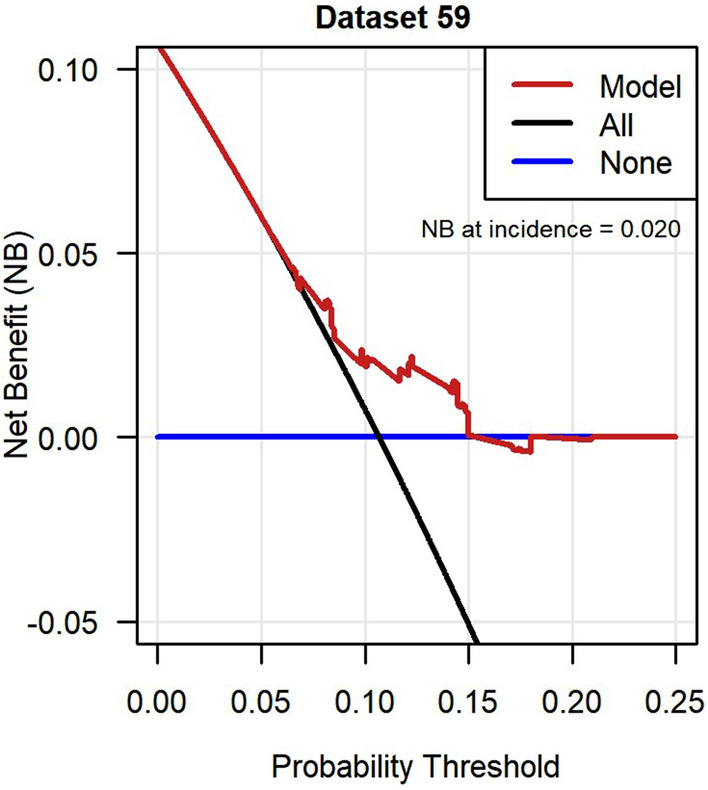
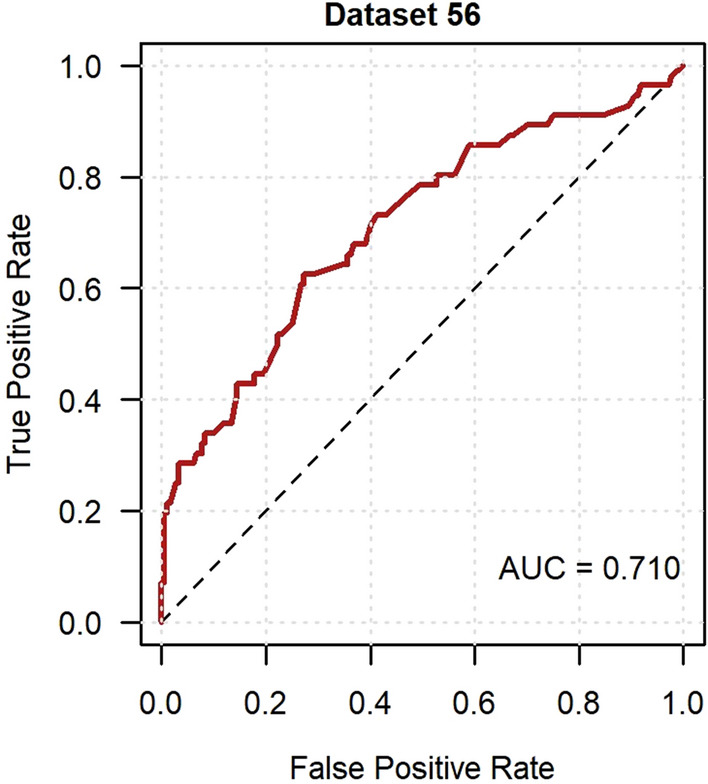
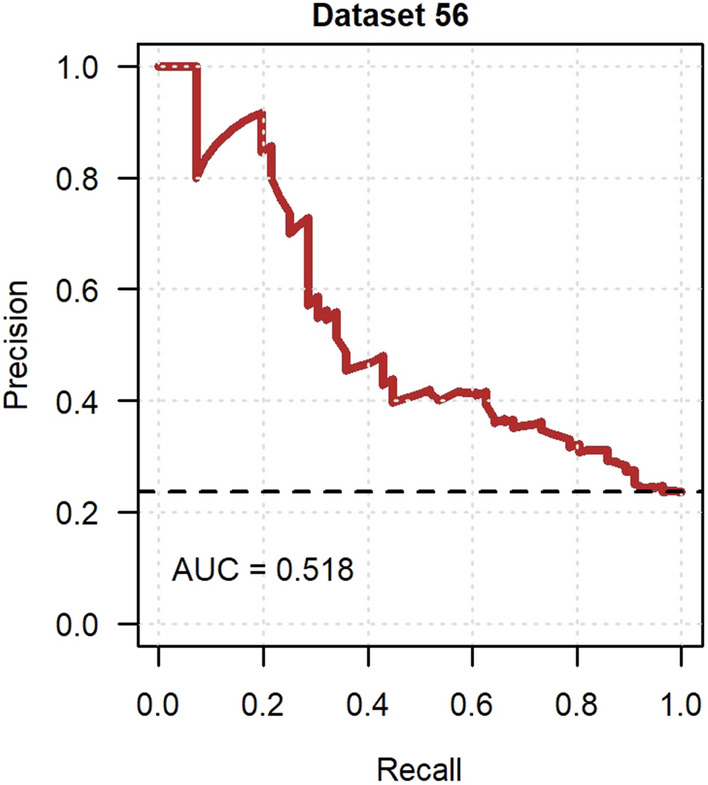
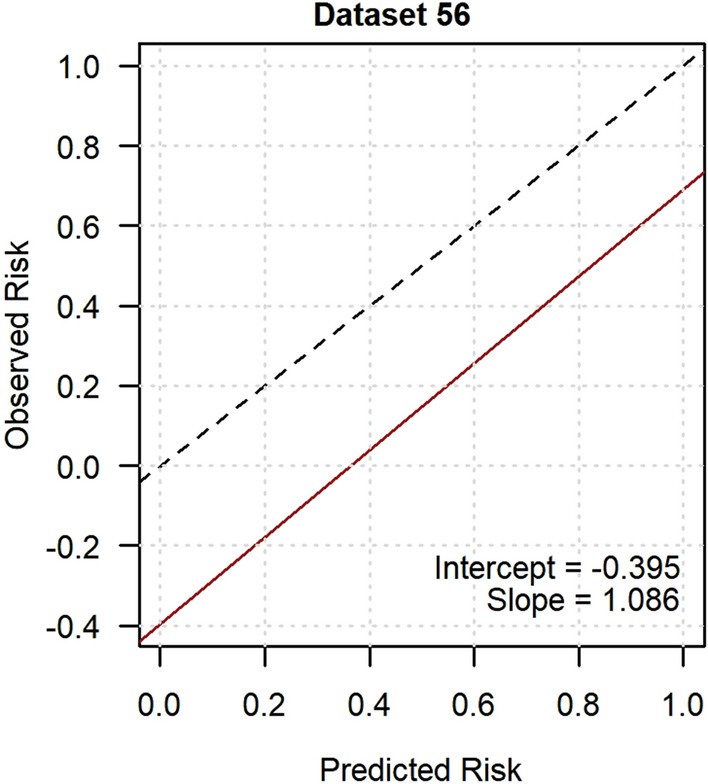
Neuropathic pain is difficult to treat, and an understanding of the risk factors for its onset and resolution is warranted. This study aimed to develop and externally validate two clinical risk models to predict onset and resolution of chronic neuropathic pain. Participants of Generation Scotland: Scottish Family Health Study (GS; general Scottish population; n = 20,221) and Genetic of Diabetes Audit and Research in Tayside Scotland (GoDARTS; n = 5236) were sent a questionnaire on neuropathic pain and followed- -up 18 months later. Chronic neuropathic pain was defined using DN4 scores (≥ 3/7) and pain for 3 months or more. The models were developed in GS using logistic regression with backward elimination based on the Akaike information criterion. External validation was conducted in GoDARTS and assessed model discrimination (ROC and Precision-Recall curves), calibration and clinical utility (decision curve analysis [DCA]). Analysis revealed incidences of neuropathic pain onset (6.0% in GS [236/3903] and 10.7% in GoDARTS [61/571]) and resolution (42.6% in GS [230/540] and 23.7% in GoDARTS [56/236]). Psychosocial and lifestyle factors were included in both onset and resolved prediction models. In GoDARTS, these models showed adequate discrimination (ROC = 0.636 and 0.699), but there was evidence of miscalibration (Intercept = - 0.511 and - 0.424; slope = 0.623 and 0.999). The DCA indicated that the models would provide clinical benefit over a range of possible risk thresholds. To our knowledge, these are the first externally validated risk models for neuropathic pain. The findings are of interest to patients and clinicians in the community, who may take preventative or remedial measures.
神经性疼痛难以治疗,因此有必要了解其发作和缓解的风险因素。本研究旨在开发和外部验证两个临床风险模型,以预测慢性神经性疼痛的发作和缓解。苏格兰基因学研究(Generation Scotland;GS;普通苏格兰人群;n=20221)和苏格兰泰赛德糖尿病审计和研究遗传学(Genetic of Diabetes Audit and Research in Tayside Scotland;GoDARTS;n=5236)的参与者收到了一份关于神经性疼痛的问卷,并在 18 个月后进行了随访。慢性神经性疼痛的定义是使用 DN4 评分(≥3/7)和疼痛持续 3 个月或以上。该模型是在 GS 中使用逻辑回归和向后消除法基于赤池信息量准则(Akaike information criterion)建立的。外部验证是在 GoDARTS 中进行的,评估了模型的区分度(ROC 和 Precision-Recall 曲线)、校准和临床实用性(决策曲线分析[DCA])。结果显示,神经性疼痛发作的发生率(GS 为 6.0%[236/3903],GoDARTS 为 10.7%[61/571])和缓解率(GS 为 42.6%[230/540],GoDARTS 为 23.7%[56/236])。心理社会和生活方式因素均包含在发作和缓解预测模型中。在 GoDARTS 中,这些模型具有较好的区分度(ROC=0.636 和 0.699),但存在校准不足的证据(截距=-0.511 和-0.424;斜率=0.623 和 0.999)。DCA 表明,这些模型在一系列可能的风险阈值范围内将提供临床获益。据我们所知,这是首次对神经性疼痛进行外部验证的风险模型。这些发现对社区中的患者和临床医生具有重要意义,他们可能会采取预防或补救措施。