EClinicalMedicine. 2025 Feb 12;81:103080. doi: 10.1016/j.eclinm.2025.103080. eCollection 2025 Mar.
Low dose corticosteroids (e.g., 6 mg dexamethasone) have been shown to reduce mortality for hypoxic COVID-19 patients. We have previously reported that higher dose corticosteroids cause harm in patients with clinical hypoxia but not receiving ventilatory support (the combination of non-invasive mechanical ventilation, including high-flow nasal oxygen, continuous positive airway pressure and bilevel positive airway pressure ventilation, and invasive mechanical ventilation or extra-corporeal membrane oxygenation), but the balance of efficacy and safety in patients receiving ventilatory support is uncertain.
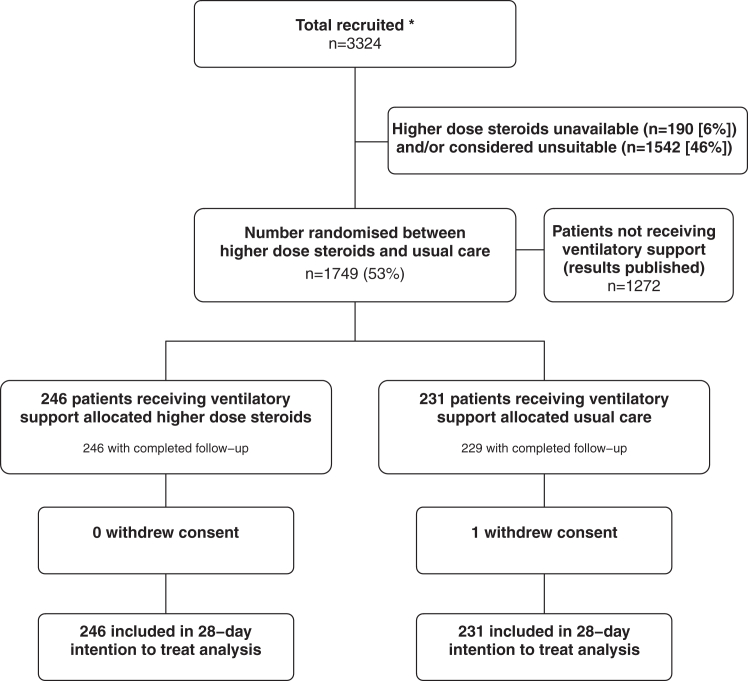
This randomised, controlled, open-label platform trial (Randomised Evaluation of COVID-19 Therapy [RECOVERY]) assessed multiple possible treatments in patients hospitalised for COVID-19. Eligible and consenting adult patients receiving ventilatory support were randomly allocated (1:1) to either usual care with higher dose corticosteroids (dexamethasone 20 mg once daily for 5 days followed by 10 mg once daily for 5 days or until discharge if sooner) or usual standard of care alone (which includes dexamethasone 6 mg once daily for 10 days or until discharge if sooner). The primary outcome was 28-day mortality; secondary outcomes were duration of hospitalisation and (among participants not on invasive mechanical ventilation at baseline) the composite of invasive mechanical ventilation or death. Recruitment closed on 31 March 2024 when funding for the trial ended. The RECOVERY trial is registered with ISRCTN (50189673) and clinicaltrials.gov (NCT04381936).
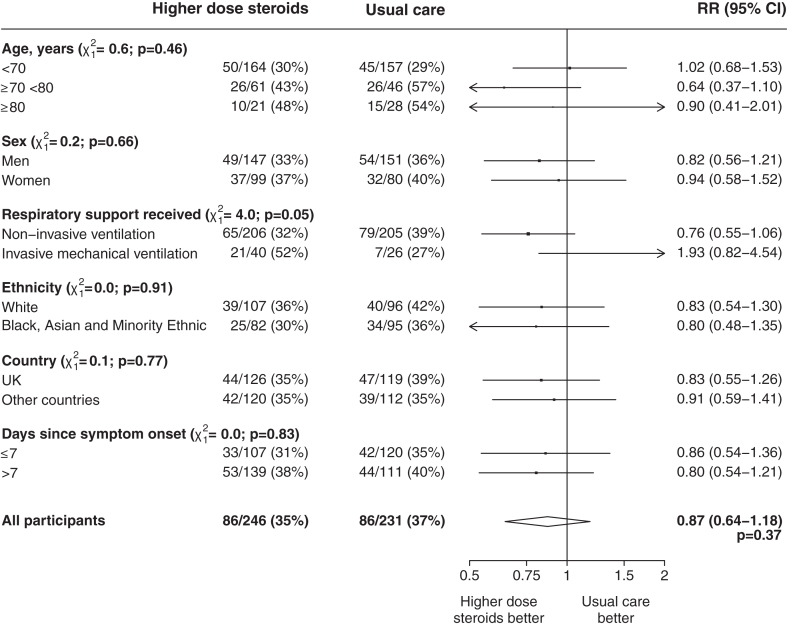
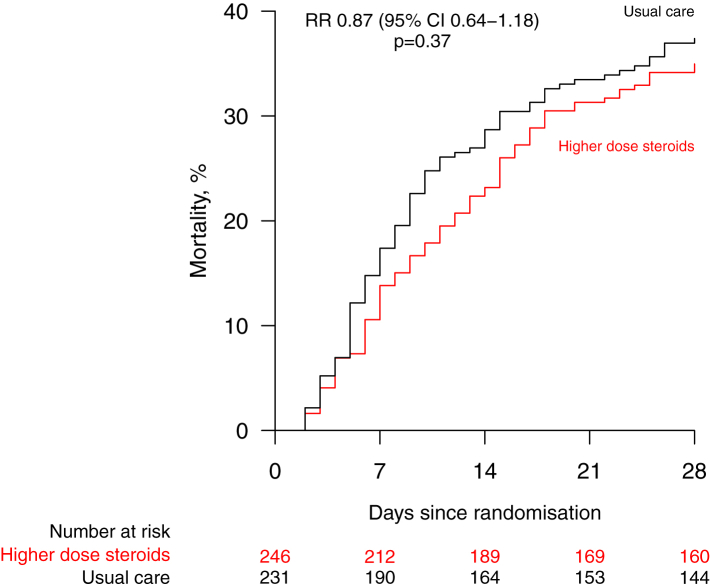
Between 25 May 2021 and 9 January 2024, 477 COVID-19 patients receiving ventilatory support were randomly allocated to receive usual care plus higher dose corticosteroids vs. usual care alone (of whom 99% received corticosteroids during the follow-up period). Of those randomised, 221 (46%) were in Asia, 245 (51%) in the UK and 11 (2%) in Africa. 143 (30%) had diabetes mellitus. Overall, 86 (35%) of 246 patients allocated to higher dose corticosteroids vs. 86 (37%) of 231 patients allocated to usual care died within 28 days (rate ratio [RR] 0.87; 95% CI 0.64-1.18; p = 0.37). There was no significant difference in the proportion of patients discharged from hospital alive within 28 days (128 [52%] in the higher dose corticosteroids group vs. 120 [52%] in the usual care group; RR 1.04, 0.81-1.33]; p = 0.78). Among those not on invasive mechanical ventilation at baseline, there was no clear reduction in the proportion meeting the composite endpoint of invasive mechanical ventilation or death (76 [37%] of 206 vs. 93 [45%] of 205; RR 0.79 [95% CI 0.63-1.00]; p = 0.05).
In patients hospitalised for COVID-19 receiving ventilatory support, we found no evidence that higher dose corticosteroids reduced the risk of death compared to usual care, which included low dose corticosteroids.
UK Research and Innovation (Medical Research Council) and National Institute for Health Research (Grant ref: MC_PC_19056), and Wellcome Trust (Grant Ref: 222406/Z/20/Z).
低剂量皮质类固醇(如6毫克地塞米松)已被证明可降低缺氧型新冠病毒疾病(COVID-19)患者的死亡率。我们之前曾报道,高剂量皮质类固醇会对临床缺氧但未接受通气支持的患者造成伤害(通气支持包括无创机械通气,如高流量鼻导管给氧、持续气道正压通气和双水平气道正压通气,以及有创机械通气或体外膜肺氧合),但接受通气支持患者的疗效和安全性平衡尚不确定。
这项随机、对照、开放标签的平台试验(新冠病毒疾病治疗随机评估[RECOVERY])评估了因COVID-19住院患者的多种可能治疗方法。符合条件并同意参与的接受通气支持的成年患者被随机分配(1:1)接受高剂量皮质类固醇的常规治疗(地塞米松20毫克,每日一次,共5天,随后10毫克,每日一次,共5天,或更早出院则停药)或仅接受常规标准治疗(包括地塞米松6毫克,每日一次,共10天,或更早出院则停药)。主要结局是28天死亡率;次要结局是住院时间以及(在基线时未接受有创机械通气的参与者中)有创机械通气或死亡的复合结局。当试验资金于2024年3月31日结束时,招募工作结束。RECOVERY试验已在国际标准随机对照试验编号注册库(ISRCTN:50189673)和美国国立医学图书馆临床试验注册库(clinicaltrials.gov:NCT04381936)注册。
在2021年5月25日至2024年1月9日期间,477名接受通气支持的COVID-19患者被随机分配接受常规治疗加高剂量皮质类固醇与仅接受常规治疗(其中99%的患者在随访期间接受了皮质类固醇治疗)。在随机分组的患者中,221名(46%)来自亚洲,245名(51%)来自英国,11名(2%)来自非洲。143名(30%)患有糖尿病。总体而言,分配至高剂量皮质类固醇组的246名患者中有86名(35%)在28天内死亡,而分配至常规治疗组的231名患者中有86名(37%)死亡(率比[RR]0.87;95%置信区间[CI]为0.64 - 1.18;p = 0.37)。28天内出院存活患者的比例无显著差异(高剂量皮质类固醇组为128名[52%],常规治疗组为120名[52%];RR 1.04,0.81 - 1.33];p = 0.78)。在基线时未接受有创机械通气的患者中,达到有创机械通气或死亡复合终点的比例没有明显降低(206名患者中有76名[37%],205名患者中有93名[45%];RR 0.79[95% CI 0.63 - 1.00];p = 0.05)。
在因COVID-19住院并接受通气支持的患者中,我们没有发现证据表明与包括低剂量皮质类固醇的常规治疗相比,高剂量皮质类固醇能降低死亡风险。
英国研究与创新署(医学研究理事会)和英国国家卫生研究院(资助编号:MC_PC_19056),以及惠康基金会(资助编号:222406/Z/20/Z)。