Chauhan Aman, Del Rivero Jaydira, Ramirez Robert A, Soares Heloisa P, Li Daneng
Division of Medical Oncology, Department of Internal Medicine, Markey Cancer Center, University of Kentucky, Lexington, KY 40536, USA.
Developmental Therapeutics Branch, National Cancer Institute, NIH, Bethesda, MD 20892, USA.
Cancers (Basel). 2022 Oct 26;14(21):5248. doi: 10.3390/cancers14215248.
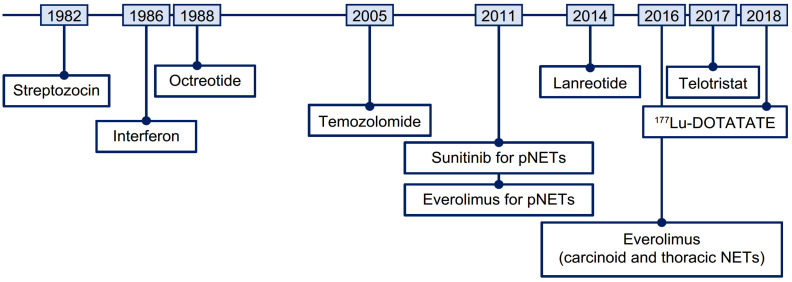
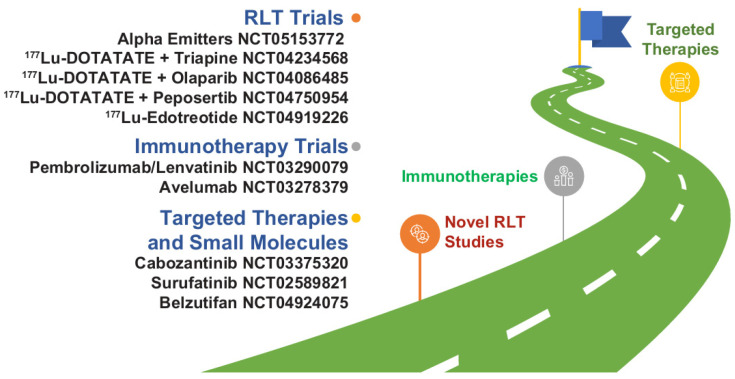
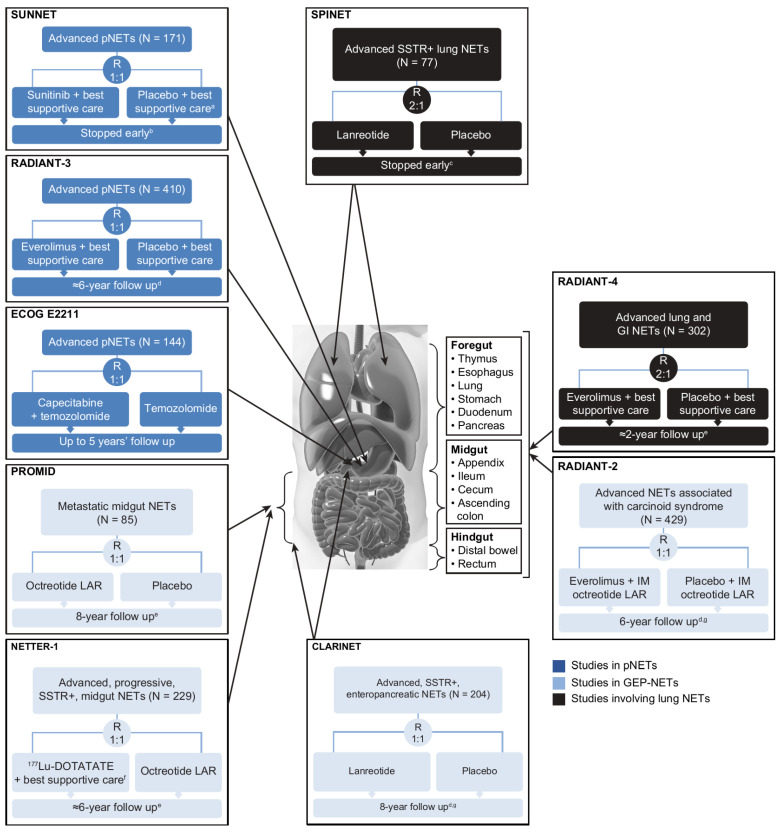
Neuroendocrine tumor (NET) incidence has grown. The treatment landscape for advanced NETs is rapidly evolving, but there are limited head-to-head data to guide treatment sequencing decisions. We assessed the available clinical data to aid practicing clinicians in their routine clinical decision-making. Clinical trials have demonstrated efficacy benefits for new therapies in advanced NETs. Emerging long-term data from these trials have enabled clinicians to make more accurate risk-benefit assessments, particularly for patients receiving multiple lines of therapy. However, clinical data specifically regarding treatment sequencing are limited. In lieu of definitive data, treatment sequencing should be based on disease-related factors (e.g., site of tumor origin, volume of disease) and patient-related characteristics (e.g., comorbidities, patient preferences). Clinical decision-making in advanced NETs remains highly individualized and complex; important evidence gaps regarding treatment sequencing remain. Given this, advanced NET management should be a joint effort of multidisciplinary teams at referring and high-volume centers. Additional clinical trial and real-world evidence are needed to meet the challenge of understanding how to sequence available NET therapies. Until these trials are conducted, the best practices provided in this review may serve as a guide for clinicians making treatment sequencing decisions based on the available data.
神经内分泌肿瘤(NET)的发病率呈上升趋势。晚期NET的治疗格局正在迅速演变,但用于指导治疗顺序决策的直接对比数据有限。我们评估了现有临床数据,以帮助执业临床医生进行常规临床决策。临床试验已证明新疗法对晚期NET具有疗效优势。这些试验中出现的长期数据使临床医生能够做出更准确的风险效益评估,特别是对于接受多线治疗的患者。然而,关于治疗顺序的具体临床数据有限。在缺乏确凿数据的情况下,治疗顺序应基于疾病相关因素(如肿瘤起源部位、疾病体积)和患者相关特征(如合并症、患者偏好)。晚期NET的临床决策仍然高度个体化且复杂;关于治疗顺序的重要证据空白仍然存在。鉴于此,晚期NET的管理应由转诊中心和大型中心的多学科团队共同努力。需要更多的临床试验和真实世界证据来应对理解如何安排现有NET疗法顺序这一挑战。在进行这些试验之前,本综述中提供的最佳实践可作为临床医生根据现有数据做出治疗顺序决策的指南。