Mahuron Kelly M, Limbach Kristen E, Hernandez Matthew C, Ituarte Philip H G, Li Daneng, Kessler Jonathan, Singh Gagandeep
Department of Surgical Oncology, City of Hope National Medical Center, Duarte, CA 91010, USA.
Department of Medical Oncology, City of Hope National Medical Center, Duarte, CA 91010, USA.
J Clin Med. 2024 Aug 23;13(17):4983. doi: 10.3390/jcm13174983.
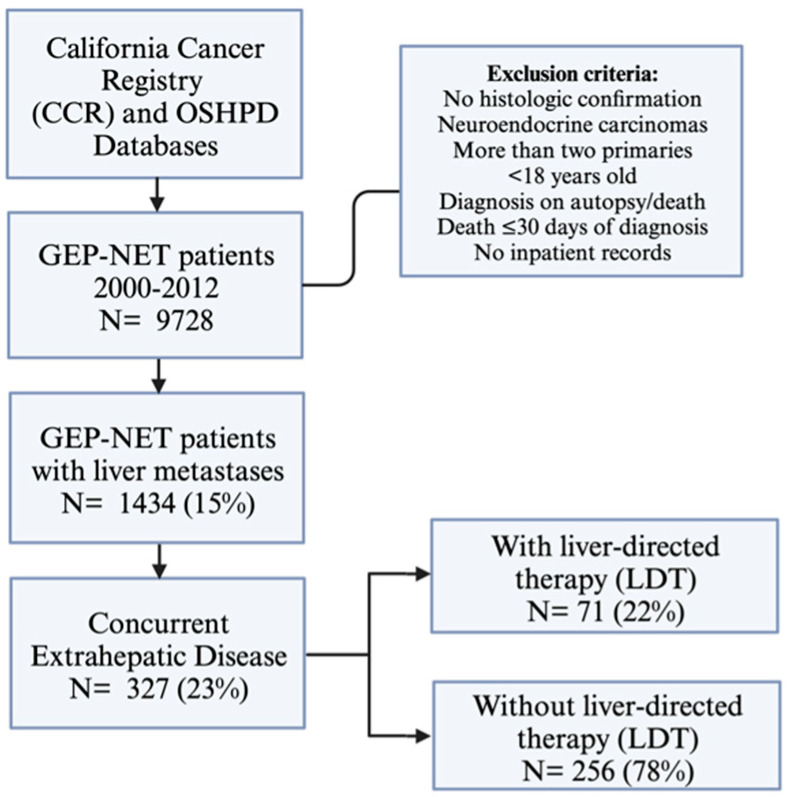
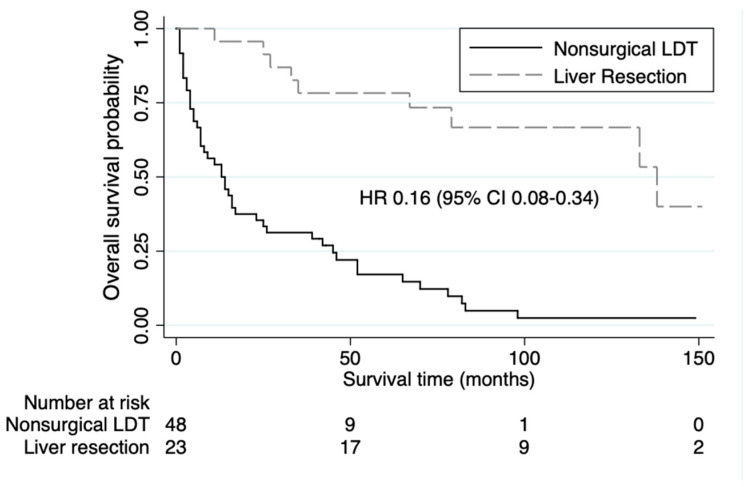
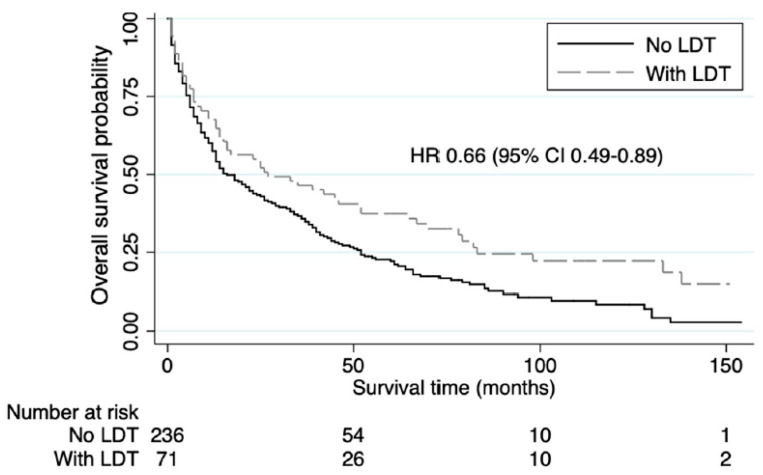
: Although survival outcomes for neuroendocrine liver metastases (NETLM) are improved with liver-direct therapies (LDT), including hepatic debulking and nonsurgical trans-arterial embolization, the benefit is less established in the setting of concurrent extrahepatic disease (EHD). We performed a population-based study to characterize the rates of LDT being performed for NETLM with EHD patients and whether LDT is associated with survival outcomes. : Patients with NETLM and EHD were identified using the California Cancer Registry database merged with data from the California Office of Statewide Health Planning and Development between 2000 and 2012. Demographics, clinical characteristics, and survival outcomes were analyzed for these patients with and without LDT. : 327 NETLM patients with EHD were identified. EHD sites included lung, peritoneum, bone, and brain. A total of 71 (22%) of these patients underwent LDT. Compared to NETLM with EHD patients who did not undergo LDT, patients who received LDT had longer median overall survival (27 vs. 16 months, = 0.006). Within the LDT group, 23 patients underwent liver resection. Liver resection was associated with longer median overall survival compared to nonsurgical LDT (138 vs. 13 months, < 0.001). : LDT candidacy should be determined for patients on a case-by-case basis, but the presence of EHD should not preclude LDT with appropriate patient selection.
尽管包括肝脏减瘤术和非手术经动脉栓塞术在内的肝脏直接治疗(LDT)改善了神经内分泌肝转移(NETLM)的生存结局,但在合并肝外疾病(EHD)的情况下,其获益尚不明确。我们进行了一项基于人群的研究,以描述对合并EHD的NETLM患者进行LDT的比例,以及LDT是否与生存结局相关。:利用加利福尼亚癌症登记数据库与2000年至2012年加利福尼亚州全州卫生规划与发展办公室的数据合并,识别出合并NETLM和EHD的患者。对这些接受和未接受LDT的患者的人口统计学、临床特征和生存结局进行了分析。:共识别出327例合并EHD的NETLM患者。EHD部位包括肺、腹膜、骨和脑。其中共有71例(22%)患者接受了LDT。与未接受LDT的合并EHD的NETLM患者相比,接受LDT的患者中位总生存期更长(27个月对16个月,P = 0.006)。在LDT组中,23例患者接受了肝切除术。与非手术LDT相比,肝切除术与更长的中位总生存期相关(138个月对13个月,P < 0.001)。:应根据具体情况为患者确定LDT的候选资格,但EHD的存在不应排除在适当选择患者的情况下进行LDT。