Department of General, Visceral and Transplantation Surgery, Ludwig-Maximilians-University Hospital Munich, Marchioninistrasse 15, 81377, Munich, Germany.
Department of Surgery, University Clinic Schleswig-Holstein Campus Luebeck, Luebeck, Germany.
BMC Surg. 2022 Nov 11;22(1):389. doi: 10.1186/s12893-022-01833-3.
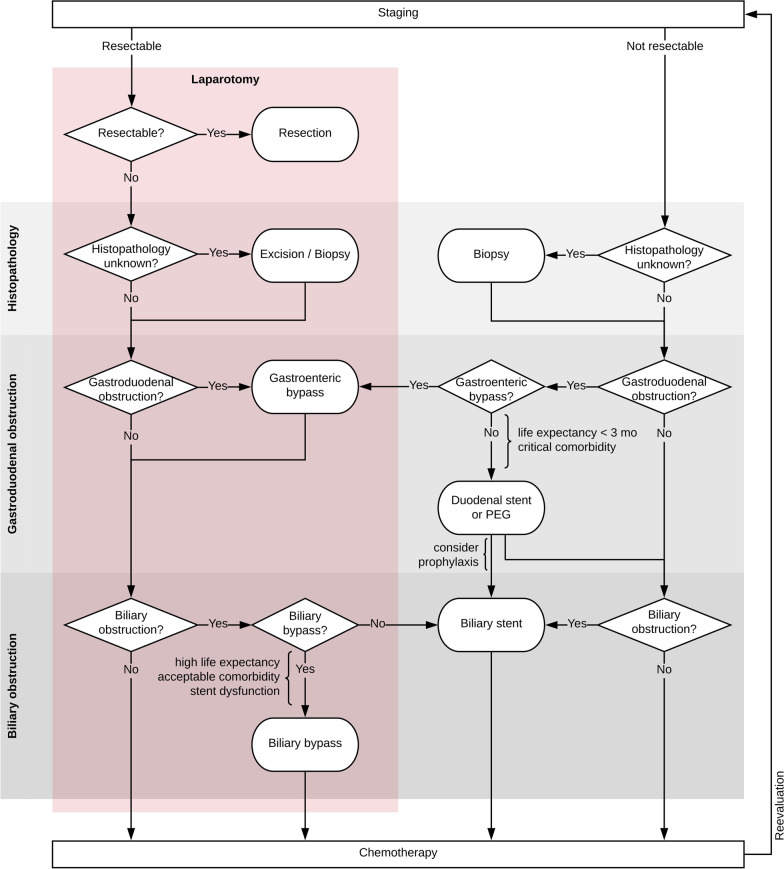
Non-resectability is common in patients with pancreatic ductal adenocarcinoma (PDAC) due to local invasion or distant metastases. Then, biliary or gastroenteric bypasses or both are often established despite associated morbidity and mortality. The current study explores outcomes after palliative bypass surgery in patients with non-resectable PDAC.
From the prospectively maintained German StuDoQ|Pancreas registry, all patients with histopathologically confirmed PDAC who underwent non-resective pancreatic surgery between 2013 and 2018 were retrospectively identified, and the influence of the surgical procedure on morbidity and mortality was analyzed.
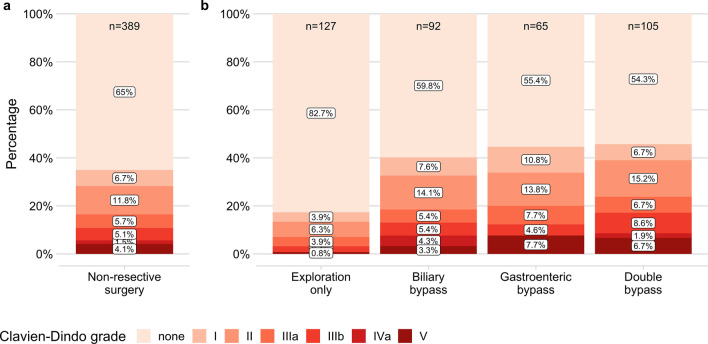
Of 389 included patients, 127 (32.6%) underwent explorative surgery only, and a biliary, gastroenteric or double bypass was established in 92 (23.7%), 65 (16.7%) and 105 (27.0%). After exploration only, patients had a significantly shorter stay in the intensive care unit (mean 0.5 days [SD 1.7] vs. 1.9 [3.6], 2.0 [2.8] or 2.1 [2.8]; P < 0.0001) and in the hospital (median 7 days [IQR 4-11] vs. 12 [10-18], 12 [8-19] or 12 [9-17]; P < 0.0001), and complications occurred less frequently (22/127 [17.3%] vs. 37/92 [40.2%], 29/65 [44.6%] or 48/105 [45.7%]; P < 0.0001). In multivariable logistic regression, biliary stents were associated with less major (Clavien-Dindo grade ≥ IIIa) complications (OR 0.49 [95% CI 0.25-0.96], P = 0.037), whereas-compared to exploration only-biliary, gastroenteric, and double bypass were associated with more major complications (OR 3.58 [1.48-8.64], P = 0.005; 3.50 [1.39-8.81], P = 0.008; 4.96 [2.15-11.43], P < 0.001).
In patients with non-resectable PDAC, biliary, gastroenteric or double bypass surgery is associated with relevant morbidity and mortality. Although surgical palliation is indicated if interventional alternatives are inapplicable, or life expectancy is high, less invasive options should be considered.
由于局部侵犯或远处转移,胰腺导管腺癌 (PDAC) 患者常出现不可切除性。尽管存在相关发病率和死亡率,但通常会建立胆道或胃肠旁路或两者兼而有之。目前的研究探讨了不可切除的 PDAC 患者姑息性旁路手术后的结果。
从前瞻性维护的德国 StuDoQ|Pancreas 登记处中,回顾性地确定了 2013 年至 2018 年间接受非切除术性胰腺手术的所有经组织病理学证实为 PDAC 的患者,并分析了手术程序对发病率和死亡率的影响。
在纳入的 389 名患者中,127 名(32.6%)仅接受了探查性手术,92 名(23.7%)、65 名(16.7%)和 105 名(27.0%)建立了胆道、胃肠或双旁路。仅探查后,患者在重症监护病房的停留时间明显缩短(平均 0.5 天 [SD 1.7] 与 1.9 [3.6]、2.0 [2.8] 或 2.1 [2.8];P < 0.0001)和住院时间(中位数 7 天 [IQR 4-11] 与 12 [10-18]、12 [8-19] 或 12 [9-17];P < 0.0001),并发症发生率较低(22/127 [17.3%] 与 37/92 [40.2%]、29/65 [44.6%] 或 48/105 [45.7%];P < 0.0001)。在多变量逻辑回归中,胆道支架与较少的主要(Clavien-Dindo 分级≥IIIa)并发症相关(OR 0.49 [95%CI 0.25-0.96],P = 0.037),而与仅探查相比,胆道、胃肠和双旁路与更多的主要并发症相关(OR 3.58 [1.48-8.64],P = 0.005;3.50 [1.39-8.81],P = 0.008;4.96 [2.15-11.43],P < 0.001)。
在不可切除的 PDAC 患者中,胆道、胃肠或双旁路手术与相关发病率和死亡率相关。尽管如果介入选择不适用或预期寿命较长,则需要进行手术姑息治疗,但应考虑更微创的选择。