Department of Cardiology and Vascular Medicine, Soetomo General Hospital, Surabaya, Indonesia.
Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia.
Am J Case Rep. 2022 Nov 14;23:e936985. doi: 10.12659/AJCR.936985.
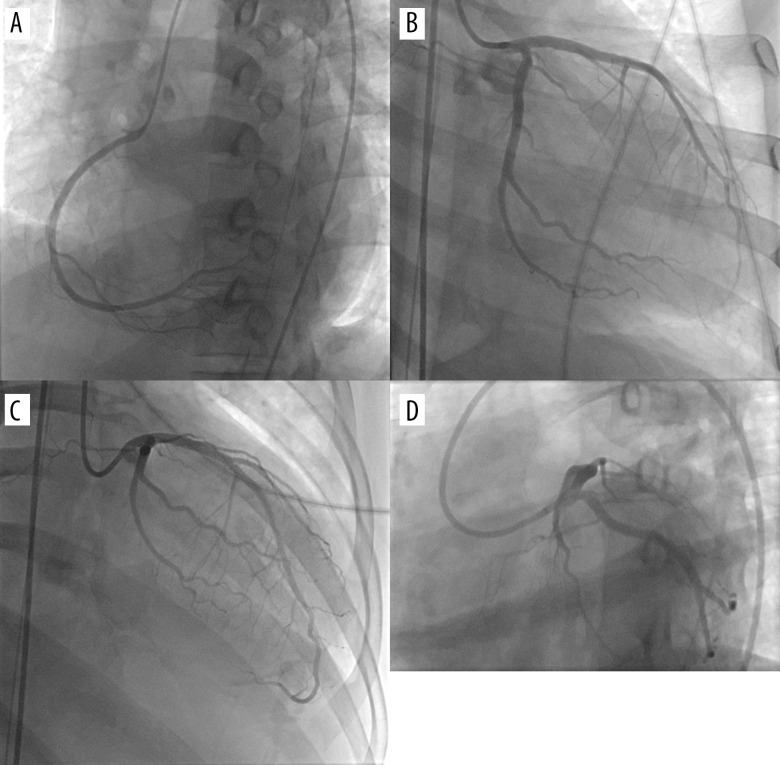
BACKGROUND A normal coronary angiogram in ST-elevation myocardial infarction (STEMI) can be considered a myocardial infarction with non-obstructive coronary arteries (MINOCA) until an alternative diagnosis is obtained. However, the COVID-19 pandemic might delay urgent coronary angiography in a resource-limited setting. Perimyocarditis often causes symptoms, such as chest pain, as well as ST-elevation and high cardiac troponin levels. This STEMI mimicker can also cause cardiogenic shock and death when not treated properly. CASE REPORT A 40-year-old man reported having acute onset of substernal chest pain, which was suspected to be STEMI. The patient was an active smoker without any risk factors or a history of cardiovascular disease. The examination showed elevated cardiac troponin I, ST-elevation in high lateral leads, and regional wall motion abnormality (RWMA) by echocardiogram. Furthermore, thrombolytic therapy had failed, and rescue percutaneous coronary intervention was not performed due to the catheterization laboratory limitation during the COVID-19 pandemic. Before coronary angiography, the patient was scheduled for 2 consecutive days of COVID-19 polymerase chain reaction (PCR) swabs. On the second day of hospitalization, the patient experienced a cardiogenic shock. The COVID-19 PCR results were negative, while coronary angiography revealed normal coronary arteries. The patient was eventually diagnosed with probable acute perimyocarditis. CONCLUSIONS Myocarditis is implicated in young patients without typical cardiovascular risk factors or in those with recent infection and cardiovascular symptoms mimicking acute coronary syndrome. It might also be present in situations where ST-elevation distribution on the electrocardiogram is discordant with the RWMA observed on the echocardiogram.
背景
在 ST 段抬高型心肌梗死(STEMI)中,如果未获得其他替代诊断,正常的冠状动脉造影可被视为非阻塞性冠状动脉心肌梗死(MINOCA)。然而,在资源有限的情况下,COVID-19 大流行可能会延迟紧急冠状动脉造影。心肌炎常引起胸痛等症状,以及 ST 段抬高和高心脏肌钙蛋白水平。如果治疗不当,这种 STEMI 模拟物也会导致心源性休克和死亡。
病例报告
一名 40 岁男性报告有胸骨后胸痛急性发作,疑似 STEMI。患者为活跃吸烟者,无任何危险因素或心血管疾病史。检查显示心脏肌钙蛋白 I 升高,高外侧导联 ST 段抬高,超声心动图显示区域性壁运动异常(RWMA)。此外,由于 COVID-19 大流行期间导管实验室的限制,溶栓治疗失败,未进行挽救性经皮冠状动脉介入治疗。在冠状动脉造影之前,患者连续两天接受 COVID-19 聚合酶链反应(PCR)拭子检查。住院第二天,患者发生心源性休克。COVID-19 PCR 结果为阴性,而冠状动脉造影显示正常冠状动脉。最终,患者被诊断为可能的急性心肌炎。
结论
心肌炎发生于无典型心血管危险因素的年轻患者,或近期感染且心血管症状模拟急性冠状动脉综合征的患者。在心电图上 ST 段抬高分布与超声心动图上观察到的 RWMA 不一致的情况下,也可能存在心肌炎。