Department of Preventive and Restorative Dentistry, College of Dental Medicine, University of Sharjah, Sharjah, UAE.
Faculty of Dentistry, The University of Hong Kong, 34 Hospital Road, Pok Fu Lam, Hong Kong, China.
BMC Med Educ. 2022 Nov 16;22(1):794. doi: 10.1186/s12909-022-03864-z.
Delivery of clinical dental education, as opposed to clinical medicine, is particularly challenging due to the obligatory aerosol-generating procedures (AGPs) used in dentistry, which are known to facilitate the spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Hence, using AGPs and working in close proximity to patients for extended periods in dental hospital/university settings with multiple teaching clinics have been a formidable prospect for all stake holders. Therefore, several professional and governmental organizations have promulgated variations of infection control guidelines for general practice dentistry in the pandemic era to mitigate SARS-CoV-2 transmission.
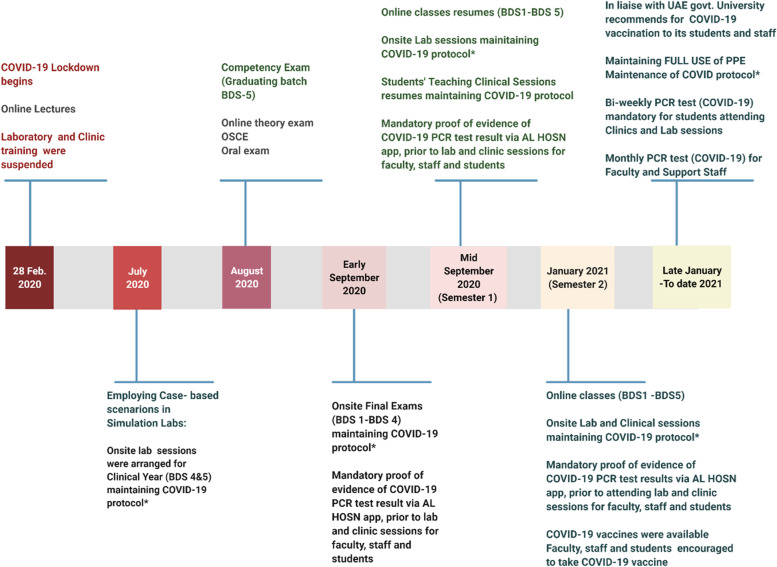
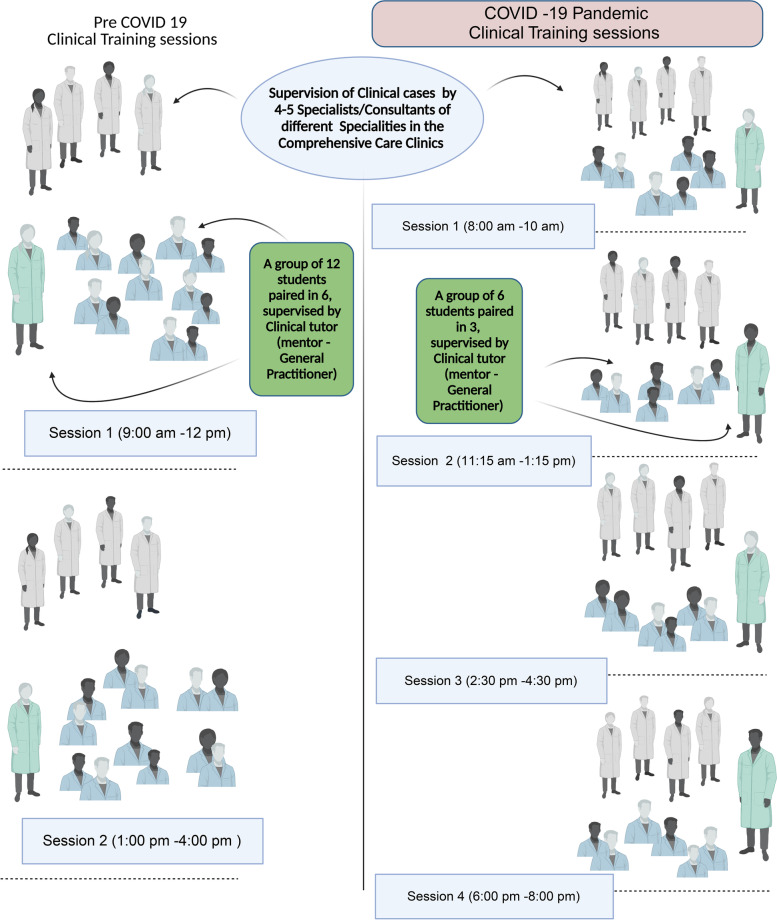
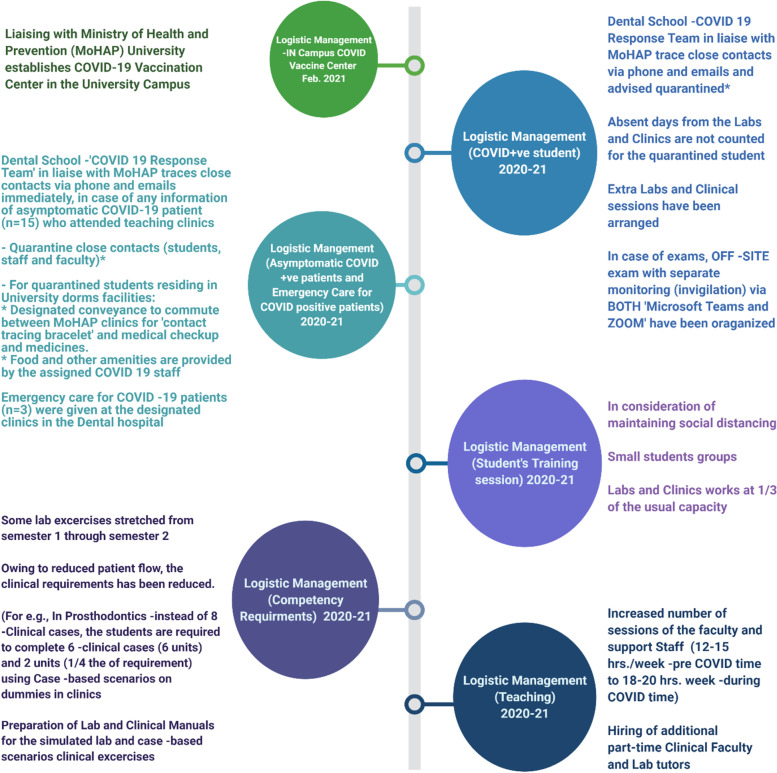
In the absence of unified guidelines for modified infection control/clinical procedures for dental education. We implemented a clinical protocol template and modified operating procedures (MOP) for teaching clinical dentistry to fit the infection control requirements during the pandemic/post-pandemic period at the Sharjah University, College of Dentistry, UAE. MOPs ranged from various engineering control measures (e.g., negative-pressure ventilation systems in operatories) to administrative control measures featuring post-procedure fallow periods of treatment-abeyance between patient sessions.
The new MOPs for clinical dentistry in the COVID-19 pandemic era, trialled in a UAE dental teaching hospital, have successfully eliminated infection transmission amongst the students, clinicians, ancillary staff, or attending patients, thus far.
The proposed MOPs that complement the standard operating protocols in clinical dentistry were an attempt to mitigate nosocomial infection transmission and protect four different groups of stakeholders, i) the patients, ii) the dental students, iii) the clinical academics, and iv) the para-dental personnel/assistants. Due to the endemicity of the COVID-19 in many regions of the World, the suggested MOPs need periodic review and revision, to fit the emerging data on the disease. Finally, as there are no studies to date comparing the relative efficacy of the MOPs in various dental academic institutions, there is an urgent need for future workers to address this issue.
与临床医学不同,临床牙科教育具有挑战性,因为牙科中使用的强制性气溶胶产生程序(AGP)已知会促进严重急性呼吸系统综合症冠状病毒 2(SARS-CoV-2)的传播。因此,在牙科医院/大学环境中,使用 AGP 并长时间近距离接触患者,并且在多个教学诊所中工作,这对所有利益相关者来说都是一个艰巨的挑战。因此,在大流行期间,为了减轻 SARS-CoV-2 的传播,一些专业和政府组织发布了针对普通牙科实践的感染控制指南的变体。
在缺乏针对牙科教育修改后的感染控制/临床程序的统一指南的情况下。我们在阿联酋沙迦大学牙科医学院实施了临床方案模板和修改后的操作程序(MOP),以适应大流行/大流行后期期间的感染控制要求。MOP 范围从各种工程控制措施(例如,诊室中的负压通风系统)到行政控制措施,包括在患者之间的治疗暂停期间。
在阿联酋牙科教学医院试行的 COVID-19 大流行时代的新牙科临床 MOP 迄今已成功消除了学生、临床医生、辅助人员或就诊患者之间的感染传播。
拟议的 MOP 补充了牙科临床标准操作程序,旨在减轻医院感染的传播并保护四类不同的利益相关者,即 i)患者,ii)牙科学生,iii)临床学者,和 iv)辅助牙科人员/助理。由于 COVID-19 在世界许多地区的流行,建议的 MOP 需要定期审查和修订,以适应该疾病的新出现数据。最后,由于迄今为止尚无研究比较各种牙科学术机构中 MOP 的相对效果,因此迫切需要未来的工作者来解决这个问题。