Department of Infection Biology, London School of Hygiene and Tropical Medicine, London, United Kingdom.
Division of Foodborne, Waterborne, and Environmental Diseases, United States Centers for Disease Control and Prevention, Atlanta, GA, United States.
Front Public Health. 2022 Oct 25;10:924316. doi: 10.3389/fpubh.2022.924316. eCollection 2022.
Infectious diseases continue to burden populations in Malaysia, especially among rural communities where resources are limited and access to health care is difficult. Current epidemiological trends of several neglected tropical diseases in these populations are at present absent due to the lack of habitual and efficient surveillance. To date, various studies have explored the utility of serological multiplex beads to monitor numerous diseases simultaneously. We therefore applied this platform to assess population level exposure to six infectious diseases in Sabah, Malaysia. Furthermore, we concurrently investigated demographic and spatial risk factors that may be associated with exposure for each disease.
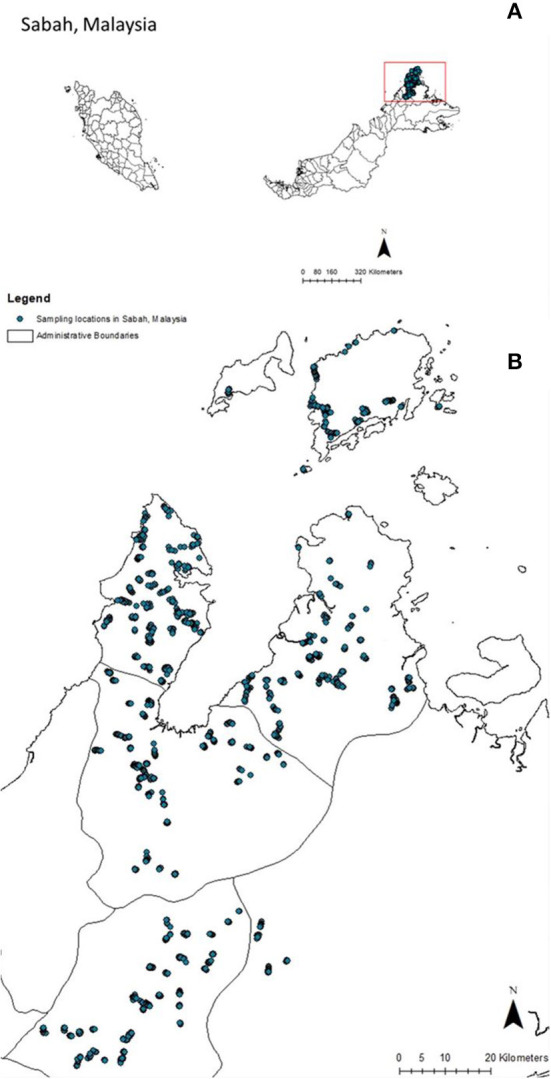
This study was conducted in four districts of Northern Sabah in Malaysian Borneo, using an environmentally stratified, population-based cross-sectional serological survey targeted to determine risk factors for malaria. Samples were collected between September to December 2015, from 919 villages totaling 10,100 persons. IgG responses to twelve antigens of six diseases (lymphatic filariasis- Bm33, Bm14, BmR1, Wb123; strongyloides- NIE; toxoplasmosis-SAG2A; yaws- Rp17 and TmpA; trachoma- Pgp3, Ct694; and giardiasis- VSP3, VSP5) were measured using serological multiplex bead assays. Eight demographic risk factors and twelve environmental covariates were included in this study to better understand transmission in this community.
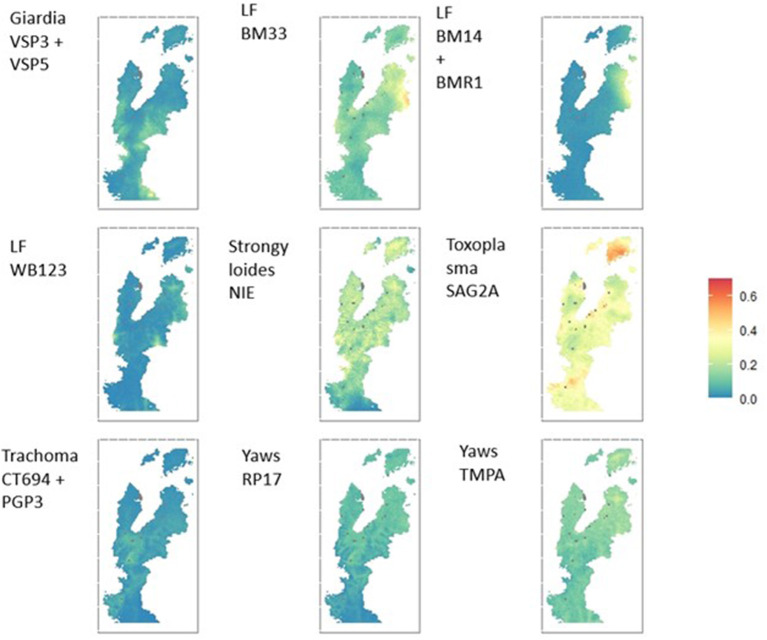
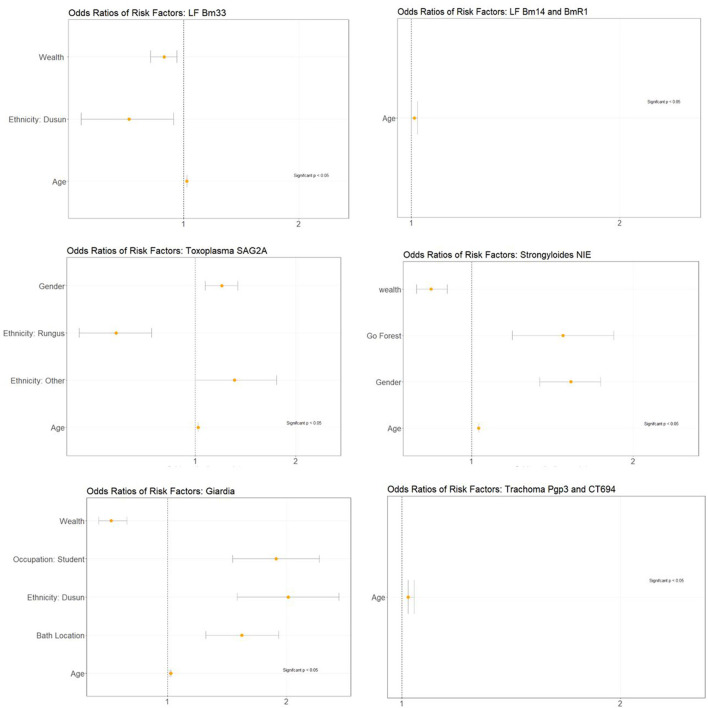
Seroprevalence of LF antigens included Bm33 (10.9%), Bm14+ BmR1 (3.5%), and Wb123 (1.7%). Seroprevalence of Strongyloides antigen NIE was 16.8%, for Toxoplasma antigen SAG2A was 29.9%, and Giardia antigens GVSP3 + GVSP5 was 23.2%. Seroprevalence estimates for yaws Rp17 was 4.91%, for TmpA was 4.81%, and for combined seropositivity to both antigens was 1.2%. Seroprevalence estimates for trachoma Pgp3 + Ct694 were 4.5%. Age was a significant risk factors consistent among all antigens assessed, while other risk factors varied among the different antigens. Spatial heterogeneity of seroprevalence was observed more prominently in lymphatic filariasis and toxoplasmosis.
Multiplex bead assays can be used to assess serological responses to numerous pathogens simultaneously to support infectious disease surveillance in rural communities, especially where prevalences estimates are lacking for neglected tropical diseases. Demographic and spatial data collected alongside serosurveys can prove useful in identifying risk factors associated with exposure and geographic distribution of transmission.
传染病继续给马来西亚的人们带来负担,尤其是在农村社区,那里资源有限,获得医疗保健的机会也很困难。目前,由于缺乏习惯性和有效的监测,这些人群中几种被忽视的热带病的当前流行病学趋势尚不存在。迄今为止,各种研究已经探索了使用血清学多重珠来同时监测多种疾病的实用性。因此,我们将该平台应用于评估马来西亚沙巴州的六种传染病的人群水平暴露情况。此外,我们还同时调查了可能与每种疾病暴露相关的人口统计学和空间危险因素。
本研究在马来西亚婆罗洲北沙巴的四个地区进行,采用环境分层的、基于人群的横断面血清学调查,旨在确定疟疾的危险因素。样本于 2015 年 9 月至 12 月间采集,来自 919 个村庄,共 10100 人。使用血清学多重珠分析来测量六种疾病的 12 种抗原的 IgG 反应(淋巴丝虫病-Bm33、Bm14+BmR1、Wb123;旋毛虫病-NIE;弓形体病-SAG2A;雅司病-Rp17 和TmpA;沙眼-Pgp3、Ct694;和贾第虫病-VSP3、VSP5)。本研究纳入了 8 个人口统计学危险因素和 12 个环境协变量,以更好地了解该社区的传播情况。
淋巴丝虫病抗原的血清阳性率包括 Bm33(10.9%)、Bm14+BmR1(3.5%)和 Wb123(1.7%)。旋毛虫病抗原 NIE 的血清阳性率为 16.8%,弓形体病抗原 SAG2A 为 29.9%,贾第虫病抗原 GVSP3+GVSP5 为 23.2%。雅司病 Rp17 的血清阳性率估计值为 4.91%,TmpA 为 4.81%,两种抗原同时呈阳性的估计值为 1.2%。沙眼 Pgp3+Ct694 的血清阳性率估计值为 4.5%。年龄是所有评估抗原中一致的重要危险因素,而其他危险因素在不同抗原中有所不同。在淋巴丝虫病和弓形体病中观察到血清阳性率的空间异质性更为明显。
多重珠分析可用于同时评估对多种病原体的血清反应,以支持农村社区的传染病监测,特别是在缺乏被忽视的热带病流行率估计值的情况下。与血清学调查一起收集的人口统计学和空间数据可用于确定与暴露相关的危险因素以及传播的地理分布。