Qin Yin, Qiu Shuting, Liu Xiaoying, Xu Shangwen, Wang Xiaoyang, Guo Xiaoping, Tang Yuting, Li Hui
Department of Rehabilitation Medicine, The 900th Hospital of Joint Logistic Support Force, People's Liberation Army (PLA), Fuzhou, China.
Department of Rehabilitation Medicine, Fuzong Clinical Medical College of Fujian Medical University, Fuzhou, China.
Front Aging Neurosci. 2022 Oct 25;14:1011812. doi: 10.3389/fnagi.2022.1011812. eCollection 2022.
The efficacy of clinical interventions for post-stroke spasticity (PSS) has been consistently unsatisfactory, probably because lesions causing PSS may occur at different locations in the brain, leaving the neuroanatomical substrates of spasticity unclear. Here, we investigated whether heterogeneous lesions causing PSS were localized to a common brain network and then identified the key nodes in this network.
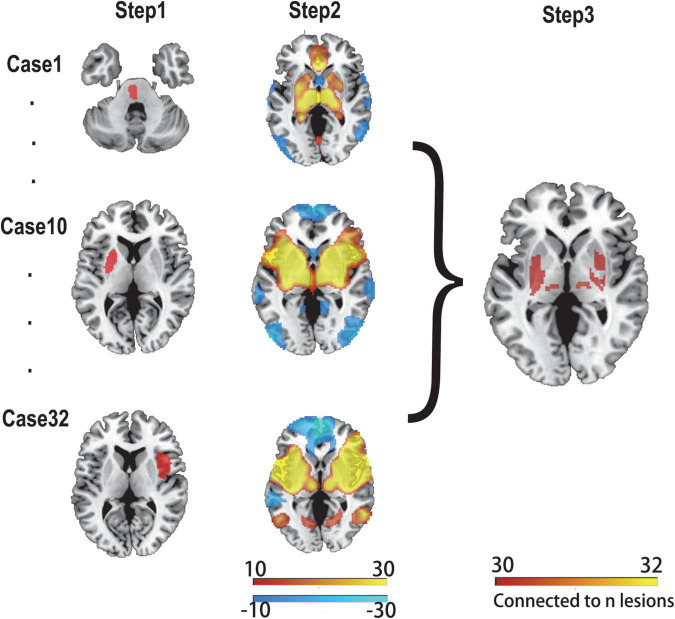
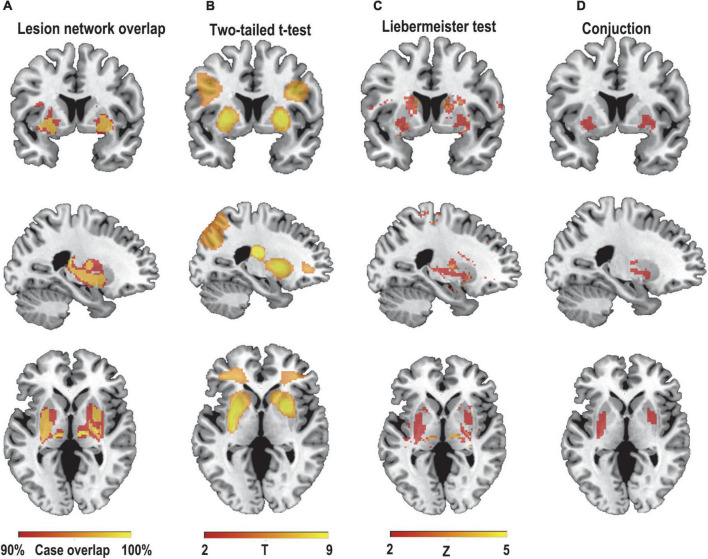
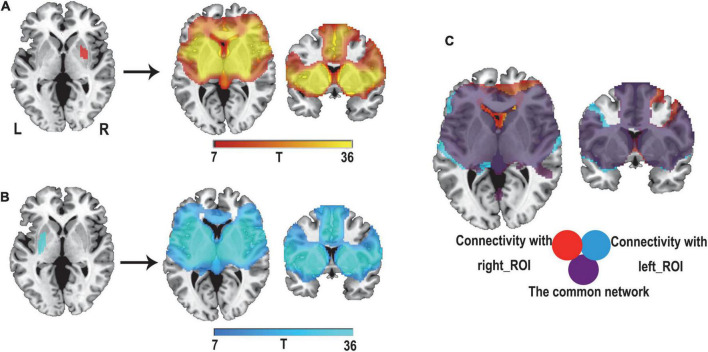
We used 32 cases of PSS and the Human Connectome dataset ( = 1,000), using a lesion network mapping method to identify the brain regions that were associated with each lesion in patients with PSS. Functional connectivity maps of all lesions were overlaid to identify common connectivity. Furthermore, a split-half replication method was used to evaluate reproducibility. Then, the lesion network mapping results were compared with those of patients with post-stroke non-spastic motor dysfunction ( = 29) to assess the specificity. Next, both sensitive and specific regions associated with PSS were identified using conjunction analyses, and the correlation between these regions and PSS was further explored by correlation analysis.
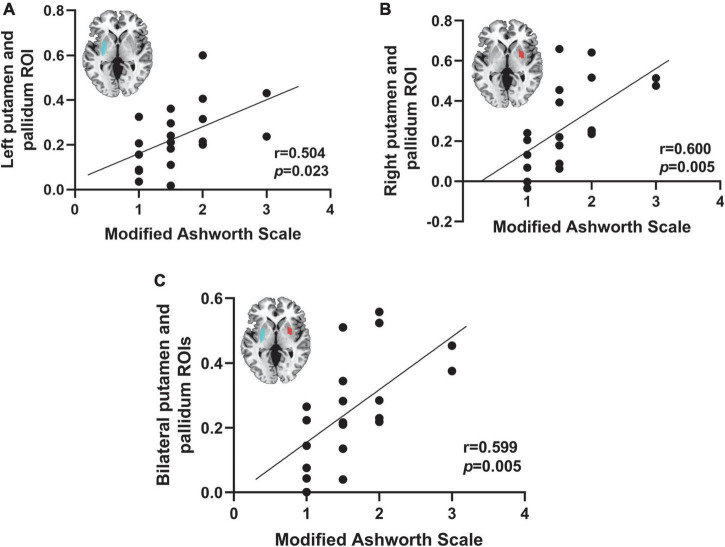
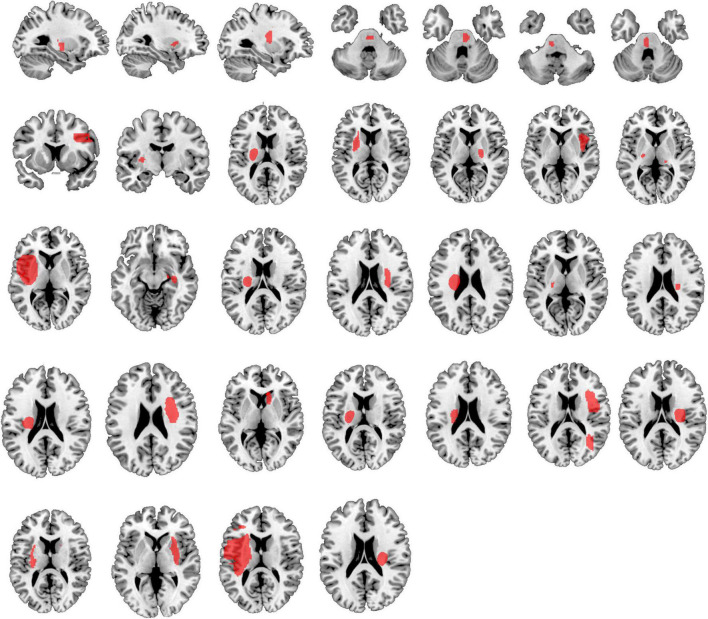
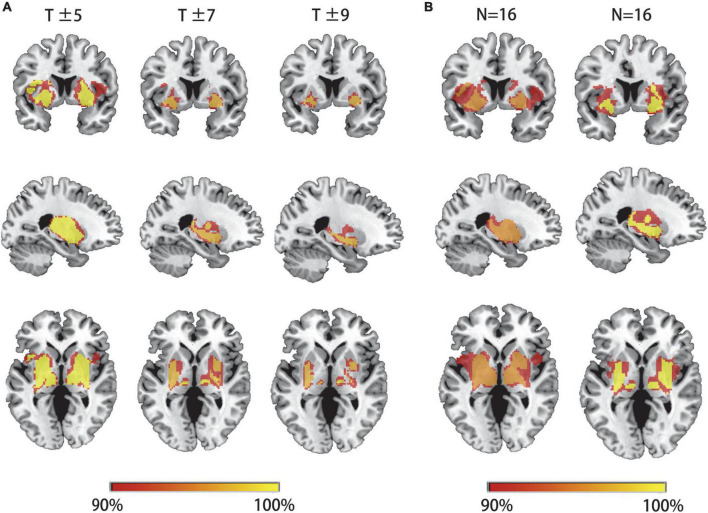
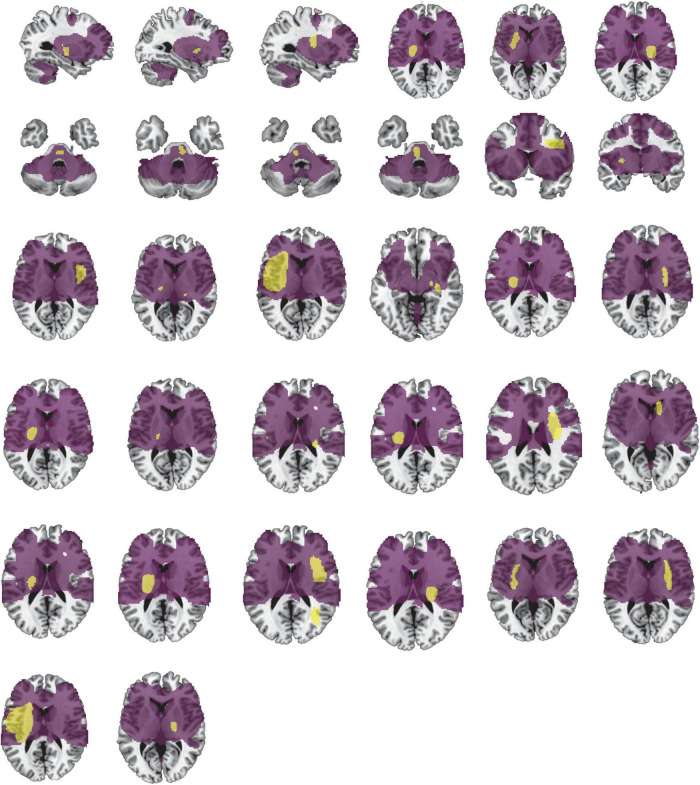
The lesions in all patients with PSS were located in different cortical and subcortical locations. However, at least 93% of these lesions (29/32) had functional connectivity with the bilateral putamen and globus pallidus. These connections were highly repeatable and specific, as compared to those in non-spastic patients. In addition, the functional connectivity between lesions and bilateral putamen and globus pallidus in patients with PSS was positively correlated with the degree of spasticity.
We identified that lesions causing PSS were localized to a common functional connectivity network defined by connectivity to the bilateral putamen and globus pallidus. This network may best cover the locations of lesions causing PSS. The putamen and globus pallidus may be potential key regions in PSS. Our findings complement previous neuroimaging studies on PSS, contributing to identifying patients with stroke at high risk for spasticity at an early stage, and may point to PSS-specific brain stimulation targets.
中风后痉挛(PSS)临床干预的疗效一直不尽人意,可能是因为导致PSS的病变可能发生在大脑的不同位置,使得痉挛的神经解剖学基础尚不清楚。在此,我们研究了导致PSS的异质性病变是否定位于一个共同的脑网络,然后确定该网络中的关键节点。
我们使用了32例PSS患者和人类连接组数据集(n = 1000),采用病变网络映射方法来确定PSS患者中与每个病变相关的脑区。将所有病变的功能连接图叠加以识别共同的连接性。此外,采用对半复制方法评估可重复性。然后,将病变网络映射结果与中风后非痉挛性运动功能障碍患者(n = 29)的结果进行比较,以评估特异性。接下来,使用联合分析确定与PSS相关的敏感和特异区域,并通过相关分析进一步探讨这些区域与PSS之间的相关性。
所有PSS患者的病变位于不同的皮质和皮质下位置。然而,这些病变中至少93%(29/32)与双侧壳核和苍白球有功能连接。与非痉挛患者相比,这些连接具有高度的可重复性和特异性。此外,PSS患者病变与双侧壳核和苍白球之间的功能连接与痉挛程度呈正相关。
我们确定导致PSS的病变定位于一个由与双侧壳核和苍白球的连接所定义的共同功能连接网络。该网络可能最能涵盖导致PSS的病变位置。壳核和苍白球可能是PSS中的潜在关键区域。我们的发现补充了先前关于PSS的神经影像学研究,有助于早期识别有痉挛高风险的中风患者,并可能指出PSS特异性的脑刺激靶点。