School of Medicine and Surgery, University of Milano-Bicocca, Milan, Italy.
Department of Infectious Diseases, San Gerardo Hospital, Monza, Italy.
Front Immunol. 2022 Oct 28;13:933960. doi: 10.3389/fimmu.2022.933960. eCollection 2022.
PTX3 is an important mediator of inflammation and innate immunity. We aimed at assessing its prognostic value in a large cohort of patients hospitalized with COVID-19.
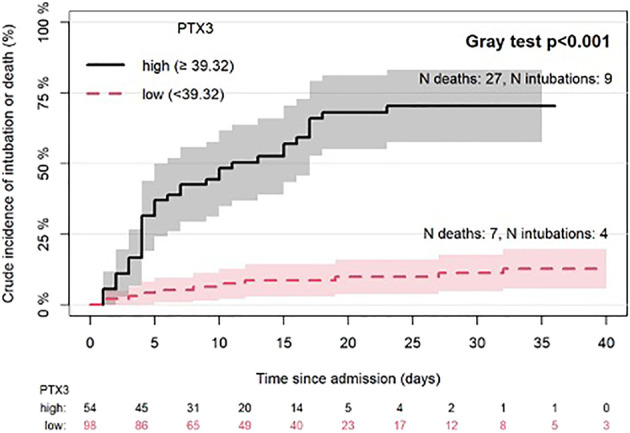
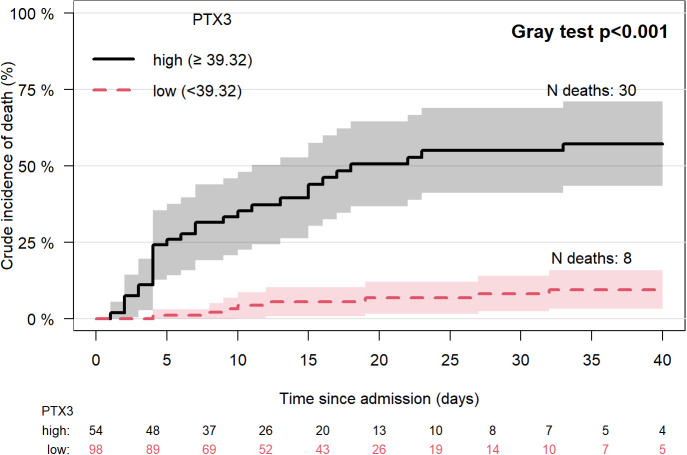
Levels of PTX3 were measured in 152 patients hospitalized with COVID-19 at San Gerardo Hospital (Monza, Italy) since March 2020. Cox regression was used to identify predictors of time from admission to in-hospital death or mechanical ventilation. Crude incidences of death were compared between patients with PTX3 levels higher or lower than the best cut-off estimated with the Maximally Selected Rank Statistics Method.
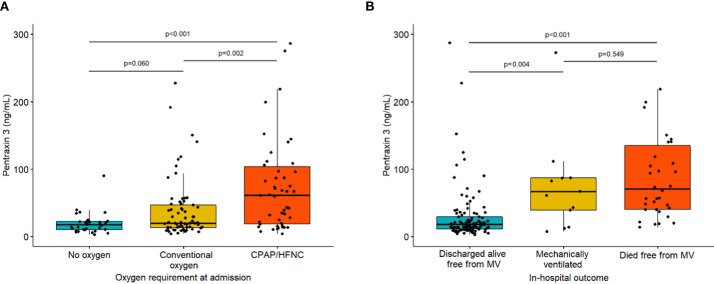
Upon admission, 22% of the patients required no oxygen, 46% low-flow oxygen, 30% high-flow nasal cannula or CPAP-helmet and 3% MV. Median level of PTX3 was 21.7 (IQR: 13.5-58.23) ng/ml. In-hospital mortality was 25% (38 deaths); 13 patients (8.6%) underwent MV. PTX3 was associated with risk of death (per 10 ng/ml, HR 1.08; 95%CI 1.04-1.11; P<0.001) and death/MV (HR 1.04; 95%CI 1.01-1.07; P=0.011), independently of other predictors of in-hospital mortality, including age, Charlson Comorbidity Index, D-dimer and C-reactive protein (CRP). Patients with PTX3 levels above the optimal cut-off of 39.32 ng/ml had significantly higher mortality than the others (55% vs 8%, P<0.001). Higher PTX3 plasma levels were found in 14 patients with subsequent thrombotic complications (median [IQR]: 51.4 [24.6-94.4] 21 [13.4-55.2]; P=0.049).
High PTX3 levels in patients hospitalized with COVID-19 are associated with a worse outcome. The evaluation of this marker could be useful in prognostic stratification and identification of patients who could benefit from immunomodulant therapy.
PTX3 是炎症和先天免疫的重要介质。我们旨在评估其在大量 COVID-19 住院患者中的预后价值。
自 2020 年 3 月以来,在意大利蒙扎圣杰尔达医院(San Gerardo Hospital)住院的 152 例 COVID-19 患者中测量了 PTX3 水平。Cox 回归用于确定从入院到院内死亡或机械通气的时间的预测因子。使用最大选择秩统计方法估计最佳截止值后,比较 PTX3 水平较高或较低的患者的死亡率。
入院时,22%的患者无需吸氧,46%的患者低流量吸氧,30%的患者高流量鼻导管或 CPAP 头盔,3%的患者需要机械通气。PTX3 的中位水平为 21.7(IQR:13.5-58.23)ng/ml。院内死亡率为 25%(38 例死亡);13 名患者(8.6%)接受了 MV。PTX3 与死亡风险相关(每增加 10ng/ml,HR 1.08;95%CI 1.04-1.11;P<0.001)和死亡/MV(HR 1.04;95%CI 1.01-1.07;P=0.011),独立于其他院内死亡率预测因子,包括年龄、Charlson 合并症指数、D-二聚体和 C 反应蛋白(CRP)。PTX3 水平高于 39.32ng/ml 最佳截断值的患者死亡率明显高于其他患者(55%比 8%,P<0.001)。在随后发生血栓并发症的 14 名患者中发现了更高的 PTX3 血浆水平(中位数 [IQR]:51.4 [24.6-94.4] 21 [13.4-55.2];P=0.049)。
COVID-19 住院患者中 PTX3 水平升高与预后不良相关。评估该标志物可用于预后分层和确定可能受益于免疫调节剂治疗的患者。