Interventional Therapy Center for Oncology, Beijing You 'an Hospital, Capital Medical University, Beijing, China.
Center for Infectious Diseases, Beijing You 'an Hospital, Capital Medical University, Beijing, China.
Front Immunol. 2022 Oct 28;13:1019772. doi: 10.3389/fimmu.2022.1019772. eCollection 2022.
Locoregional interventional therapy including transcatheter arterial chemoembolization (TACE) and ablation are the current standard of treatment for early-to-mid-stage hepatocellular carcinoma (HCC). However, questions remain unanswered regarding the management of recurrence after locoregional treatment. PD-1 inhibitors can block inhibitory signals of T-cell activation and proliferation to reduce the recurrence. We conducted a single-arm phase 2 trial to evaluate the efficacy and safety of PD-1 inhibitors following locoregional interventional therapy in HCC patients with high recurrence risk guided by our novel scoring system.
Patients enrolled initially treated by TACE combined with ablation, then willingly joined the experimental group. One month later, they received the anti-PD-1 adjuvant therapy (intravenous injection of 200 mg), which was repeated every 3 weeks for a total of 4 or 8 cycles. Within this same period, other patients were screened into the control group to match the experimental group by 1:1 based on the propensity score matching method (PSM). The primary endpoint was relapse-free survival (RFS). Secondary endpoints included overall survival (OS) recurrence modality, safety, and quality of life.
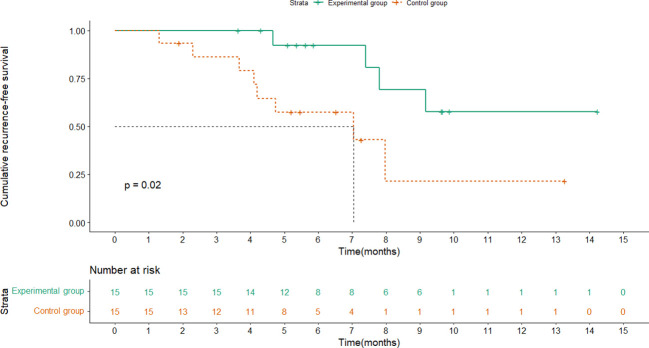
At the time of data cutoff, the median RFS of the control group was 7.0 months while the experimental group had not reached it. Moreover, the 1-year RFS rate was 73.3% in the experimental group and 46.7% in the control group, showing a significant difference (P =0.02). The rate of local tumor progression in the experimental group was clearly lower than that in the control group (P = 0.027). Benefits associated with anti-PD-1 adjuvant therapy were observed in patients with multiple tumors and tumor size ≤2cm. Univariate and multivariate analyses demonstrated that anti-PD-1 adjuvant therapy was an independent favorable prognostic factor for RFS in HCC patients. The most frequent AE observed in this study was RCCEP, and other AEs included diarrhea, hepatotoxicity, rash, pruritus, and fatigue. The incidence of GRADE ≥3 AE and withdrawal in this study was low with no deaths recorded.
Interim analysis from the study suggest the addition of anti-PD-1 adjuvant therapy after TACE combined with ablation could significantly prolong RFS with controllable safety for early-to-mid-stage HCC patients with high recurrence risk.
局部介入治疗,包括经导管动脉化疗栓塞(TACE)和消融,是目前治疗早期至中期肝细胞癌(HCC)的标准治疗方法。然而,局部治疗后复发的管理仍存在一些问题。PD-1 抑制剂可以阻断 T 细胞激活和增殖的抑制信号,从而减少复发。我们进行了一项单臂 2 期临床试验,评估了我们新的评分系统指导下的局部介入治疗后 PD-1 抑制剂在高复发风险的 HCC 患者中的疗效和安全性。
患者最初接受 TACE 联合消融治疗,然后自愿加入实验组。一个月后,他们接受抗 PD-1 辅助治疗(静脉注射 200mg),每 3 周重复一次,共 4 或 8 个周期。在此期间,其他患者通过倾向评分匹配(PSM)方法按 1:1 比例筛选入对照组与实验组匹配。主要终点是无复发生存(RFS)。次要终点包括总生存(OS)、复发方式、安全性和生活质量。
数据截止时,对照组的中位 RFS 为 7.0 个月,而实验组尚未达到。此外,实验组的 1 年 RFS 率为 73.3%,对照组为 46.7%,差异有统计学意义(P=0.02)。实验组局部肿瘤进展率明显低于对照组(P=0.027)。在肿瘤多发和肿瘤直径≤2cm 的患者中观察到抗 PD-1 辅助治疗的获益。单因素和多因素分析表明,抗 PD-1 辅助治疗是 HCC 患者 RFS 的独立有利预后因素。该研究中最常见的 AE 是 RCCEP,其他 AE 包括腹泻、肝毒性、皮疹、瘙痒和疲劳。该研究中 GRADE≥3AE 的发生率和停药率较低,无死亡记录。
研究的中期分析表明,对于高复发风险的早期至中期 HCC 患者,在 TACE 联合消融后加用抗 PD-1 辅助治疗可显著延长 RFS,且安全性可控。