Department of Emergency Surgery, Lu'an Hospital of Anhui Medical University, Lu'an, China.
Department of Clinical Medicine, West Anhui Health Vocational College, Lu'an, China.
Medicine (Baltimore). 2022 Nov 18;101(46):e31671. doi: 10.1097/MD.0000000000031671.
Isotonic crystalloids are the preferred solution for the initial clinical management of patients with multiple trauma, among which lactated Ringer's solution and normal saline are the most widely used, but both have clinical limitations. Bicarbonated Ringer's solution (BRS), which provides physiological levels of bicarbonate ions and electrolyte ions, can be used to supplement missing extracellular fluid and correct metabolic acidosis.
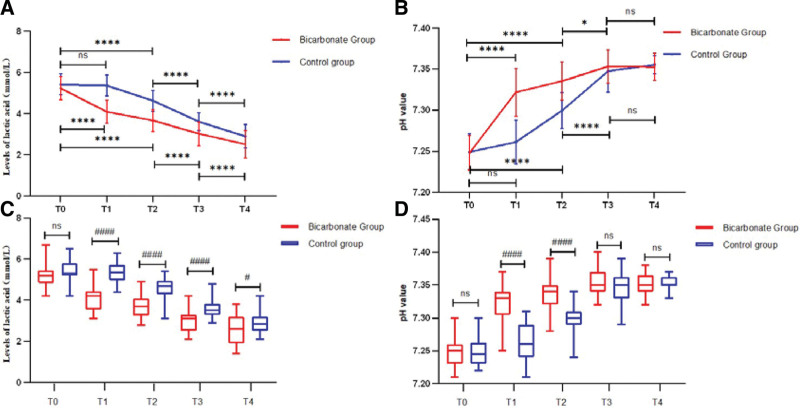
A prospective, randomized controlled study enrolled 63 patients with traumatic hepatic rupture and hemorrhagic shock. They were randomly assigned to the Bicarbonated group (n = 33) or the Control group (n = 30), which received restrictive fluid resuscitation with sodium bicarbonate Ringer's solution or sodium lactate Ringer's solution, respectively. The levels of interleukin (IL)-6, tumor necrosis factor (TNF)-α, arterial blood lactic acid and potential of hydrogen (pH) were measured prior to, 1, 3, 24, and 72 hours following resuscitation. The primary outcomes were patient survival, shock-related complications, and comparison of the inflammatory factors.
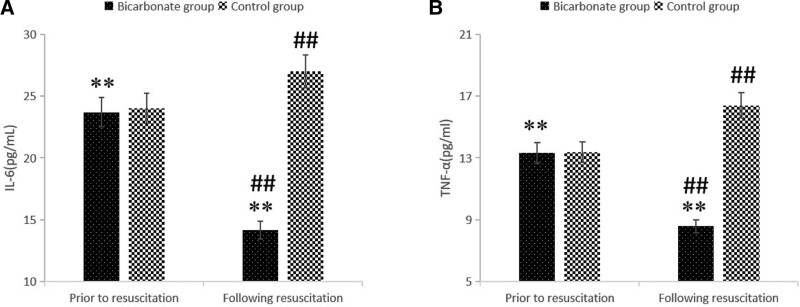
The incidence of complications in the Bicarbonated group was significantly lower than in the Control group (15.15% vs 40.0%; P < .05). The intensive care unit length of stay and mechanical ventilation time in the Bicarbonated group were significantly shorter than in the Control group (all P < .01). The levels of IL-6 and TNF-α in the Bicarbonated group were significantly lower 1 hour following resuscitation than prior to resuscitation (P < .01), whereas these levels in the Control group were increased following 1h of resuscitation as compared with before resuscitation (P < .01). Following resuscitation, the levels of IL-6, TNF-α and lactate in the Bicarbonated group were significantly lower than in the Control group (P < .01). Moreover, in the Bicarbonated group, the lactic acid level decreased and the pH value increased significantly following resuscitation, whereas there was no difference in lactic acid levels and pH value between pre- and 1 hour post-resuscitation in the Control group (P > .05).
The shock-related complications were dramatically reduced from using BRS in these patients. Additionally, the BRS was found to better inhibit the expression of inflammatory factors in their peripheral blood and could correct acidosis.
等张晶体液是治疗多发创伤患者的首选初始临床管理溶液,其中乳酸林格氏液和生理盐水的应用最为广泛,但均存在临床局限性。碳酸氢盐林格氏液(BRS)可提供生理水平的碳酸氢根离子和电解质离子,可用于补充细胞外液缺失并纠正代谢性酸中毒。
前瞻性、随机对照研究纳入了 63 例创伤性肝破裂合并失血性休克患者。他们被随机分配至碳酸氢盐组(n=33)或对照组(n=30),分别接受碳酸氢盐林格氏液或乳酸钠林格氏液进行限制性液体复苏。复苏前、复苏后 1、3、24 和 72 小时,测量白细胞介素(IL)-6、肿瘤坏死因子(TNF)-α、动脉血乳酸和 pH 值。主要结局是患者生存情况、休克相关并发症和炎症因子的比较。
碳酸氢盐组的并发症发生率明显低于对照组(15.15% vs 40.0%;P<.05)。碳酸氢盐组的 ICU 住院时间和机械通气时间明显短于对照组(均 P<.01)。碳酸氢盐组复苏后 1 小时的 IL-6 和 TNF-α水平明显低于复苏前(均 P<.01),而对照组复苏后 1 小时的这些水平较复苏前升高(均 P<.01)。复苏后,碳酸氢盐组的 IL-6、TNF-α和乳酸水平明显低于对照组(均 P<.01)。此外,碳酸氢盐组乳酸水平降低,pH 值升高,而对照组复苏前后乳酸水平和 pH 值无差异(P>.05)。
在这些患者中使用 BRS 可显著降低与休克相关的并发症。此外,BRS 还发现能更好地抑制其外周血中炎症因子的表达,并纠正酸中毒。