Department of Tropical Medicine, Medical Microbiology and Pharmacology, John A. Burns School of Medicine, University of Hawaii at Manoa, 651 Ilalo Street, Bioscience Building Suite 320, Honolulu, HI, 96813, USA.
Cancer Early Detection Advanced Research Center (CEDAR), School of Medicine, Knight Cancer Institute, Oregon Health & Science University, 2720 S. Moody Avenue, Portland, OR, USA.
Malar J. 2022 Nov 19;21(1):346. doi: 10.1186/s12936-022-04360-x.
The primary antibody (Ab) response to Plasmodium falciparum is a critical step in developing immunity to malaria. Information on the initial Ab responses of babies in malaria-endemic areas is incomplete, in part, because babies receive maternal IgG via transplacental-transfer and usually become infected before maternal IgG wanes. The study aimed to identify the primary IgM and IgG Ab responses to malarial antigens in Cameroonian babies.
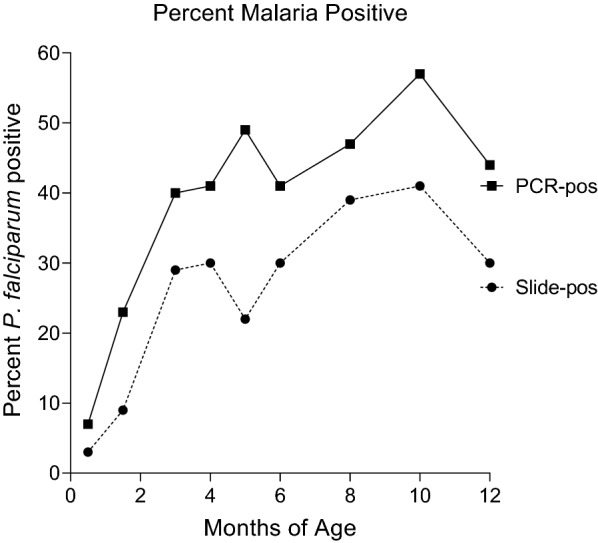
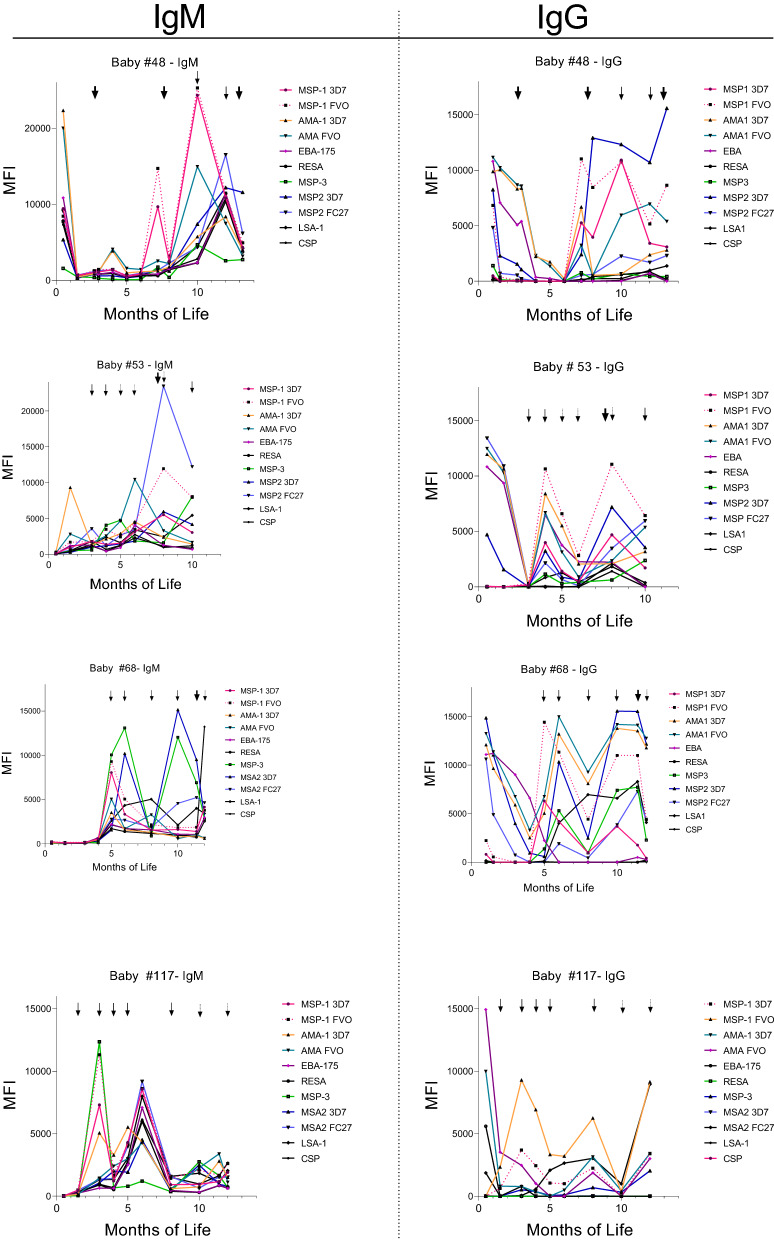
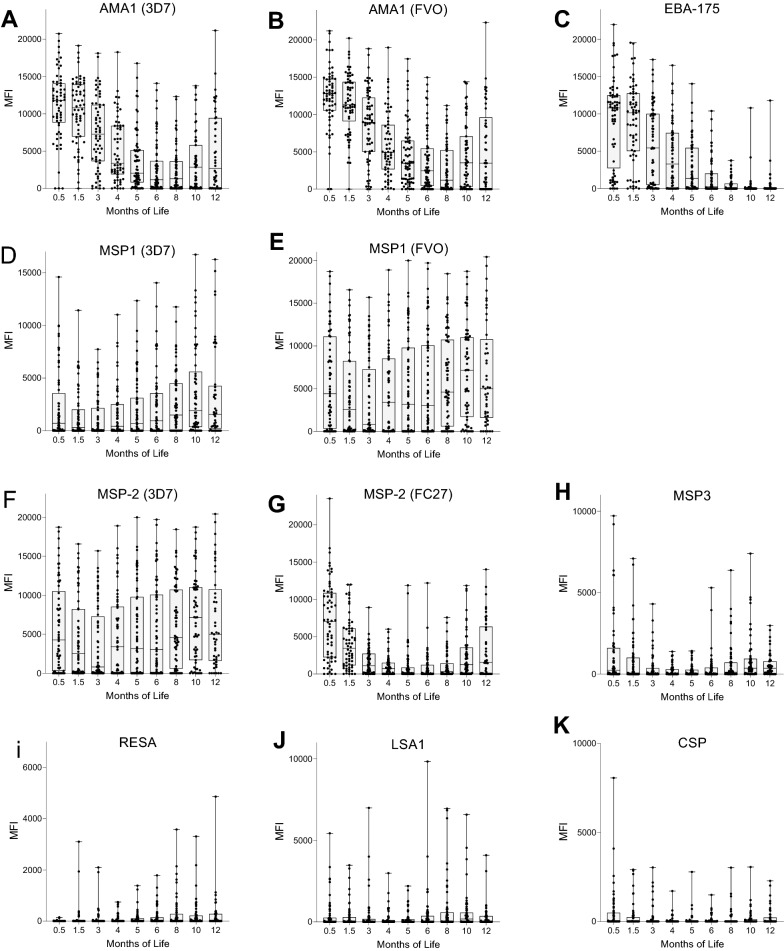
Infants (n = 70) living in a high malaria transmission area were followed from birth throughout the first year of life (mean 341 ± 42 days, an average of 8.5 time points per infant). Malaria infection was assessed by microscopy and PCR, and IgM and IgG antibodies (Abs) were measured using a multiplex immunoassay to AMA1, EBA-175, MSP1-42, MSP2, MSP3, RESA, LSA1, and CSP.
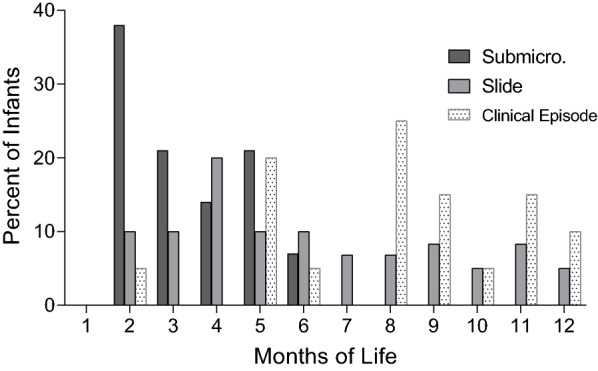
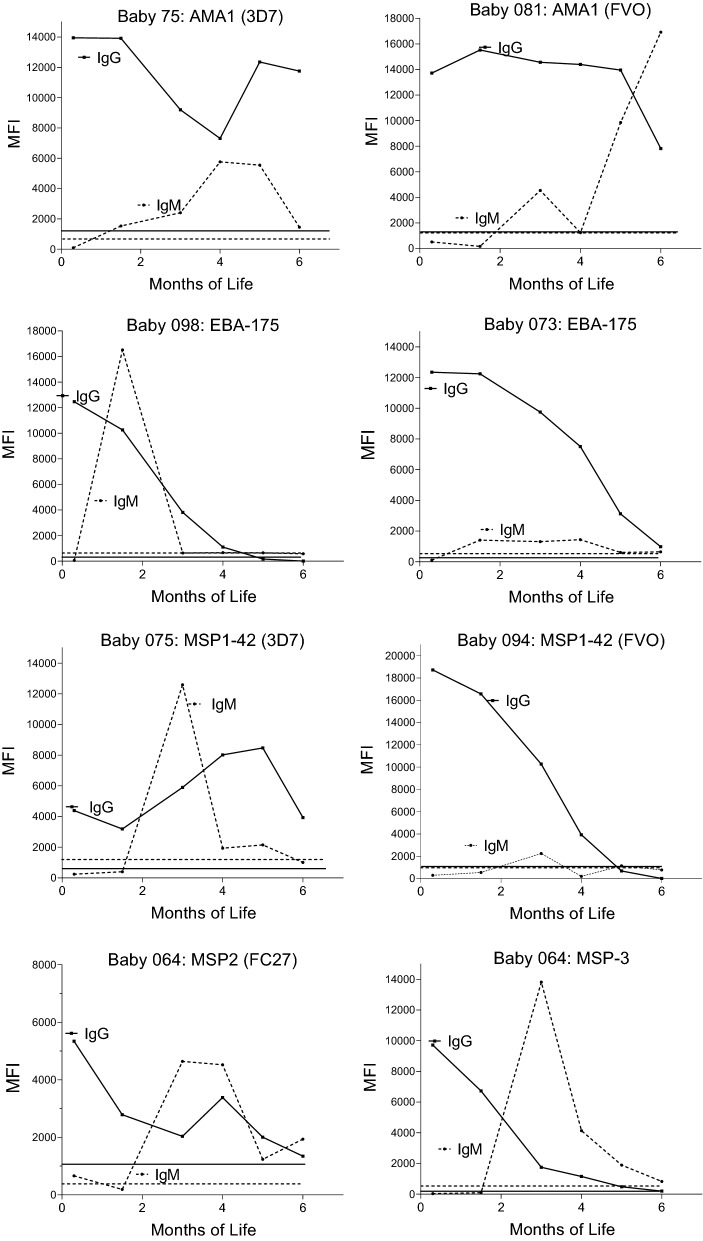
The half-life of maternal IgG varied among the antigens, ranging from 0.7 to 2.5 months. The first infection of 41% of the babies was sub-microscopic and only 11 to 44% of the babies produced IgM to the above antigens; however, when the first infection was detected by microscopy, 59-82% of the infants made IgM Abs to the antigens. Infants were able to produce IgM even when maternal IgG was present, suggesting maternal Abs did not suppress the baby's initial Ab response. Using longitudinal regression models that incorporated time-varying covariates, infants were found to produce IgG Ab to only AMA-1 when the first infection was sub-microscopic, but they produced IgG Abs to MSP1-42 (3D7, FVO), AMA1 (3D7, FVO) MSP2-FC27, MSP3, RESA, and LSA1, but not MSP 2-3D7, EBA-175, and CSP during their first slide-positive infection. Notably, the primary and secondary IgG responses were short-lived with little evidence of boosting.
The primary Ab response of babies who had maternal IgG was similar to that reported for primary infections in malaria-naïve adults.
针对恶性疟原虫的主要抗体(Ab)反应是对疟疾产生免疫力的关键步骤。在疟疾流行地区,婴儿的初始 Ab 反应信息并不完整,部分原因是婴儿通过胎盘转移接受母体 IgG,并且通常在母体 IgG 衰减之前就被感染。本研究旨在确定喀麦隆婴儿对疟原虫抗原的主要 IgM 和 IgG Ab 反应。
对生活在高疟疾传播地区的婴儿(n=70)从出生到生命的第一年进行了随访(平均 341±42 天,每个婴儿平均 8.5 个时间点)。通过显微镜检查和 PCR 评估疟疾感染,并用多重免疫测定法测量 IgM 和 IgG 抗体(Abs)以评估 AMA1、EBA-175、MSP1-42、MSP2、MSP3、RESA、LSA1 和 CSP。
母体 IgG 的半衰期因抗原而异,范围为 0.7 至 2.5 个月。41%的婴儿首次感染呈亚微观,只有 11%至 44%的婴儿对上述抗原产生 IgM;然而,当通过显微镜检测到首次感染时,59%-82%的婴儿对这些抗原产生 IgM Abs。即使存在母体 IgG,婴儿也能够产生 IgM,表明母体 Abs 并未抑制婴儿的初始 Ab 反应。使用包含时变协变量的纵向回归模型,发现当首次感染呈亚微观时,婴儿仅能产生针对 AMA-1 的 IgG Ab,但在首次镜检阳性感染时,婴儿能够产生 IgG Abs 针对 MSP1-42(3D7、FVO)、AMA1(3D7、FVO)MSP2-FC27、MSP3、RESA 和 LSA1,但不能产生针对 MSP2-3D7、EBA-175 和 CSP 的 IgG Abs。值得注意的是,主要和次要 IgG 反应的寿命较短,几乎没有增强的证据。
具有母体 IgG 的婴儿的初始 Ab 反应与先前报告的疟疾初发感染的初始 Ab 反应相似。