Leeds Institute for Medical Research, University of Leeds, Leeds, UK.
Cancer Research Clinical Trials Unit, University of Birmingham, Birmingham, UK.
Lancet Healthy Longev. 2022 Dec;3(12):e825-e838. doi: 10.1016/S2666-7568(22)00239-2. Epub 2022 Nov 17.
Older patients with early-stage rectal cancer are under-represented in clinical trials and, therefore, little high-quality data are available to guide treatment in this patient population. The TREC trial was a randomised, open-label feasibility study conducted at 21 centres across the UK that compared organ preservation through short-course radiotherapy (SCRT; 25 Gy in five fractions) plus transanal endoscopic microsurgery (TEM) with standard total mesorectal excision in adults with stage T1-2 rectal adenocarcinoma (maximum diameter ≤30 mm) and no lymph node involvement or metastasis. TREC incorporated a non-randomised registry offering organ preservation to patients who were considered unsuitable for total mesorectal excision by the local colorectal cancer multidisciplinary team. Organ preservation was achieved in 56 (92%) of 61 non-randomised registry patients with local recurrence-free survival of 91% (95% CI 84-99) at 3 years. Here, we report acute and long-term patient-reported outcomes from this non-randomised registry group.
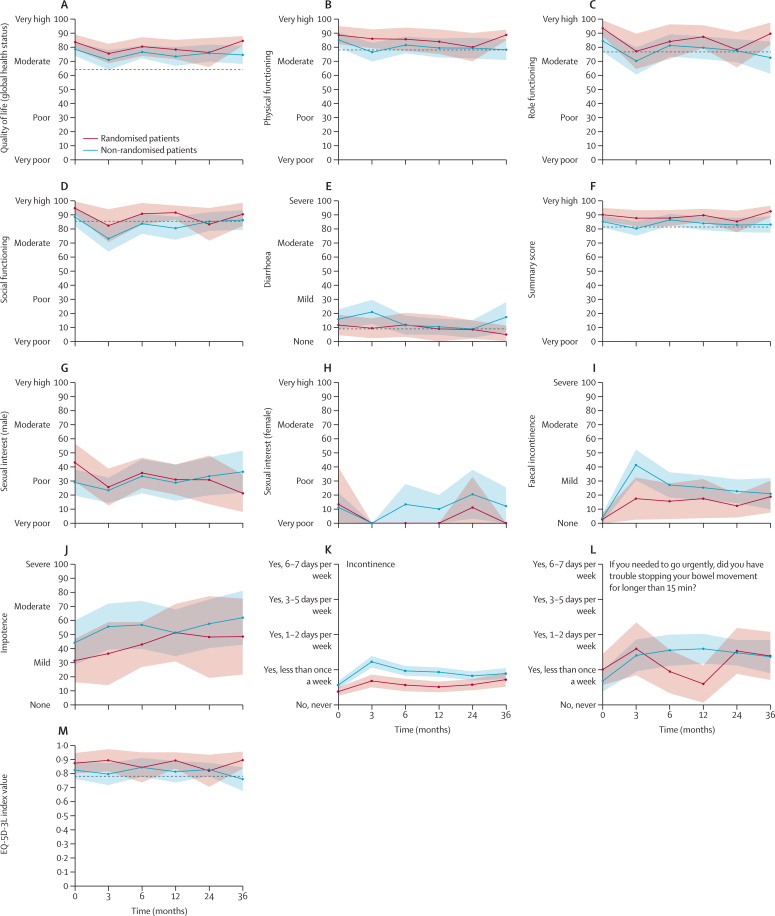
Patients considered by the local colorectal cancer multidisciplinary team to be at high risk of complications from total mesorectal excision on the basis of frailty, comorbidities, and older age were included in a non-randomised registry to receive organ-preserving treatment. These patients were invited to complete questionnaires on patient-reported outcomes (the European Organisation for Research and Treatment of Cancer Quality of Life [EORTC-QLQ] questionnaire core module [QLQ-C30] and colorectal cancer module [QLQ-CR29], the Colorectal Functional Outcome [COREFO] questionnaire, and EuroQol-5 Dimensions-3 Level [EQ-5D-3L]) at baseline and at months 3, 6, 12, 24, and 36 postoperatively. To aid interpretation, data from patients in the non-randomised registry were compared with data from those patients in the TREC trial who had been randomly assigned to organ-preserving therapy, and an additional reference cohort of aged-matched controls from the UK general population. This study is registered with the ISRCTN registry, ISRCTN14422743, and is closed.
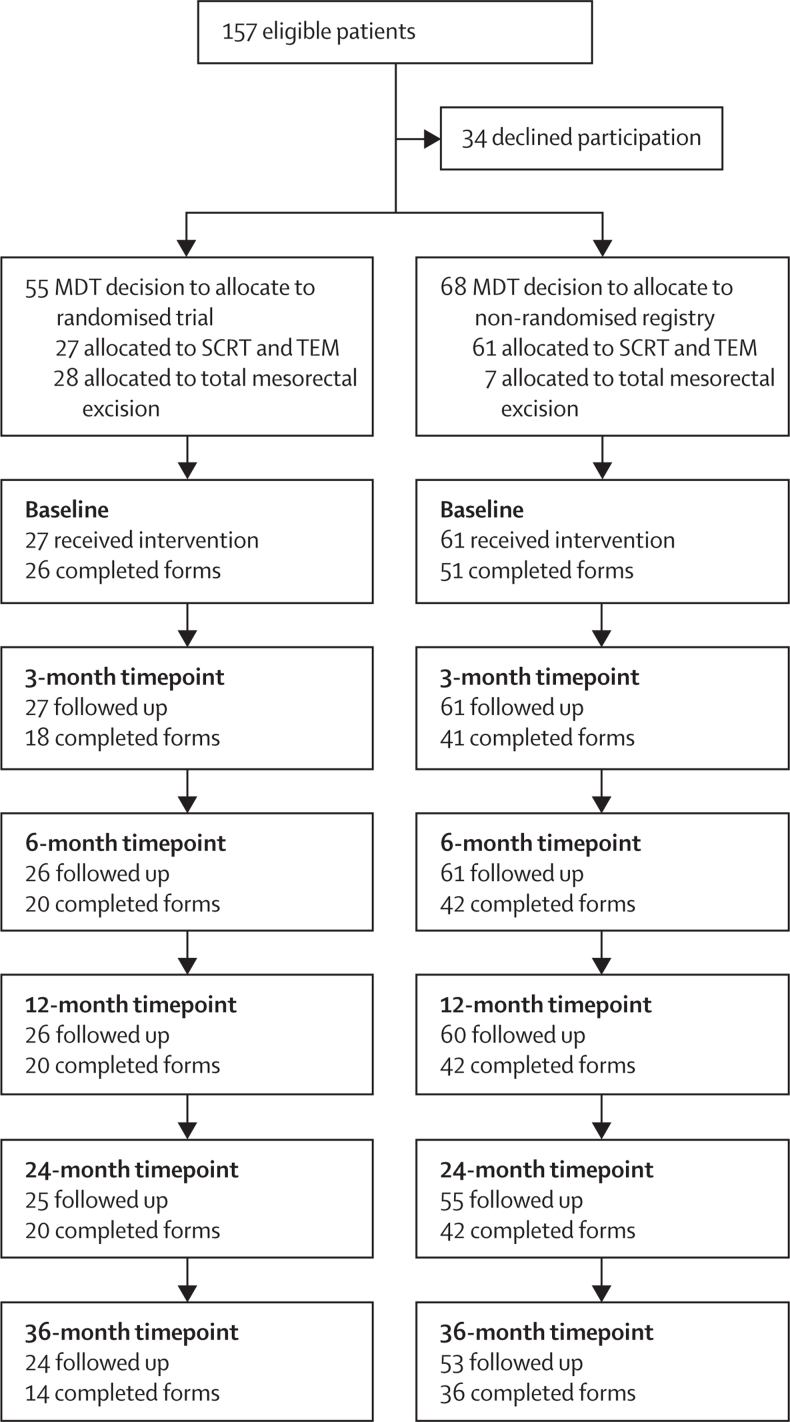
Between July 21, 2011, and July 15, 2015, 88 patients were enrolled onto the TREC study to undergo organ preservation, of whom 27 (31%) were randomly allocated to organ-preserving therapy and 61 (69%) were added to the non-randomised registry for organ-preserving therapy. Non-randomised patients were older than randomised patients (median age 74 years [IQR 67-80] vs 65 years [61-71]). Organ-preserving treatment was well tolerated among patients in the non-randomised registry, with mild worsening of fatigue; quality of life; physical, social, and role functioning; and bowel function 3 months postoperatively compared with baseline values. By 6-12 months, most scores had returned to baseline values, and were indistinguishable from data from the reference cohort. Only mild symptoms of faecal incontinence and urgency, equivalent to less than one episode per week, persisted at 36 months among patients in both groups.
The SCRT and TEM organ-preservation approach was well tolerated in older and frailer patients, showed good rates of organ preservation, and was associated with low rates of acute and long-term toxicity, with minimal effects on quality of life and functional status. Our findings support the adoption of this approach for patients considered to be at high risk from radical surgery.
Cancer Research UK.
早期直肠癌的老年患者在临床试验中代表性不足,因此,针对这一患者群体的治疗方法缺乏高质量的数据。TREC 试验是在英国 21 个中心进行的一项随机、开放性可行性研究,比较了短程放疗(SCRT;25 Gy 分 5 次)联合经肛门内镜微创手术(TEM)与标准全直肠系膜切除术在 T1-2 期直肠腺癌(最大直径≤30 mm)且无淋巴结受累或转移的成人中的器官保存效果。TREC 纳入了一个非随机登记处,为那些被当地结直肠癌多学科团队认为不适合行全直肠系膜切除术的患者提供器官保存治疗。在非随机登记处的 61 例患者中,56 例(92%)实现了器官保存,3 年时局部无复发生存率为 91%(95%CI 84-99)。在此,我们报告了来自该非随机登记组的急性和长期患者报告结局。
根据虚弱、合并症和年龄等因素,被当地结直肠癌多学科团队认为存在全直肠系膜切除术后并发症风险高的患者被纳入非随机登记处,接受器官保存治疗。这些患者被邀请在术后 3、6、12、24 和 36 个月时完成患者报告结局问卷(欧洲癌症研究与治疗组织生活质量问卷核心模块[EORTC-QLQ]、结直肠癌模块[QLQ-CR29]、结直肠功能结局问卷[COREFO]和欧洲五维健康量表[EQ-5D-3L])。为了便于解释,我们将非随机登记处患者的数据与 TREC 试验中随机分配至器官保存治疗组的患者数据进行了比较,并与来自英国普通人群的年龄匹配对照队列的数据进行了比较。本研究在 ISRCTN 注册中心(ISRCTN80653255)注册,现已关闭。
2011 年 7 月 21 日至 2015 年 7 月 15 日,有 88 例患者入组 TREC 研究接受器官保存治疗,其中 27 例(31%)随机分配至器官保存治疗组,61 例(69%)被添加至非随机登记处接受器官保存治疗。非随机登记处患者比随机登记处患者年龄更大(中位数年龄 74 岁[IQR 67-80] vs 65 岁[61-71])。非随机登记处患者的器官保存治疗耐受性良好,与基线相比,术后 3 个月时疲劳、生活质量、身体、社会和角色功能以及肠道功能出现轻度恶化。6-12 个月后,大多数评分已恢复至基线值,且与参考队列的数据无差异。两组患者在 36 个月时均仅有轻度粪便失禁和急迫感症状(每周少于 1 次)。
SCRT 和 TEM 器官保存方法在老年和虚弱患者中耐受性良好,具有较高的器官保存率,且与急性和长期毒性相关的发生率低,对生活质量和功能状态的影响最小。我们的研究结果支持为被认为有根治性手术高风险的患者采用这种方法。
英国癌症研究基金会。