Baker Heart and Diabetes Institute, Melbourne, VIC, Australia.
School of Public Health and Preventive Medicine, Monash University, Melbourne, VIC, Australia.
Diabetologia. 2023 Apr;66(4):642-656. doi: 10.1007/s00125-022-05832-0. Epub 2022 Nov 21.
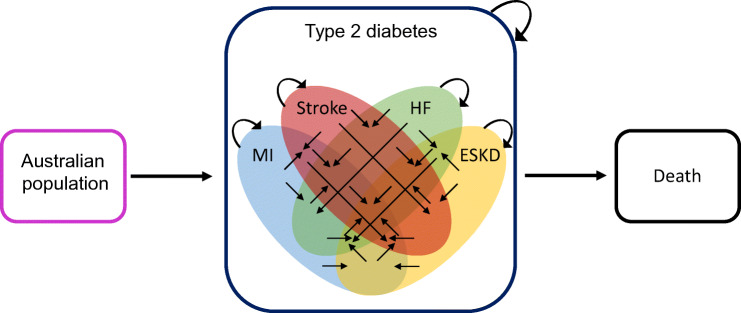
AIMS/HYPOTHESIS: Whether sodium-glucose co-transporter 2 inhibitors (SGLT2is) or glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are cost-effective based solely on their cardiovascular and kidney benefits is unknown. We projected the health and economic outcomes due to myocardial infarction (MI), stroke, heart failure (HF) and end-stage kidney disease (ESKD) among people with type 2 diabetes, with and without CVD, under scenarios of widespread use of these drugs.
We designed a microsimulation model using real-world data that captured CVD and ESKD morbidity and mortality from 2020 to 2040. The populations and transition probabilities were derived by linking the Australian Diabetes Registry (1.1 million people with type 2 diabetes) to hospital admissions databases, the National Death Index and the ESKD Registry using data from 2010 to 2019. We modelled four interventions: increase in use of SGLT2is or GLP-1 RAs to 75% of the total population with type 2 diabetes, and increase in use of SGLT2is or GLP-1 RAs to 75% of the secondary prevention population (i.e. people with type 2 diabetes and prior CVD). All interventions were compared with current use of SGLT2is (20% of the total population) and GLP-1 RAs (5% of the total population). Outcomes of interest included quality-adjusted life years (QALYs), total costs (from the Australian public healthcare perspective) and the incremental cost-effectiveness ratio (ICER). We applied 5% annual discounting for health economic outcomes. The willingness-to-pay threshold was set at AU$28,000 per QALY gained.
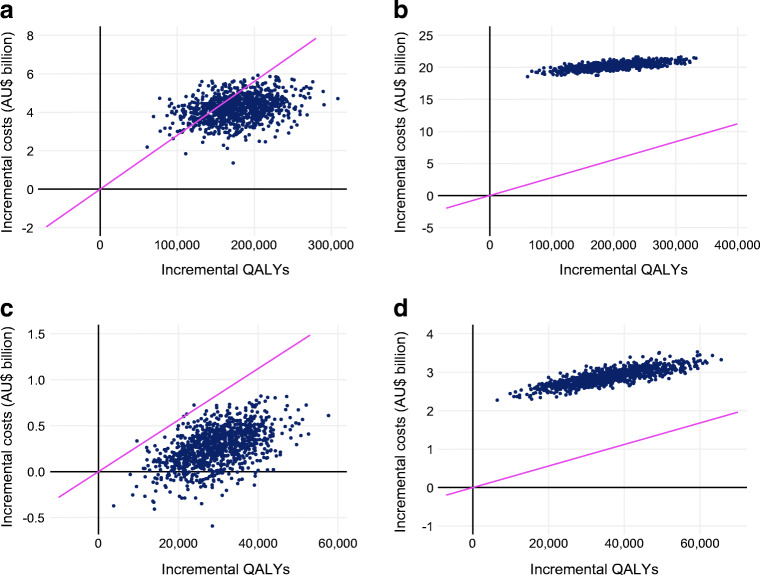
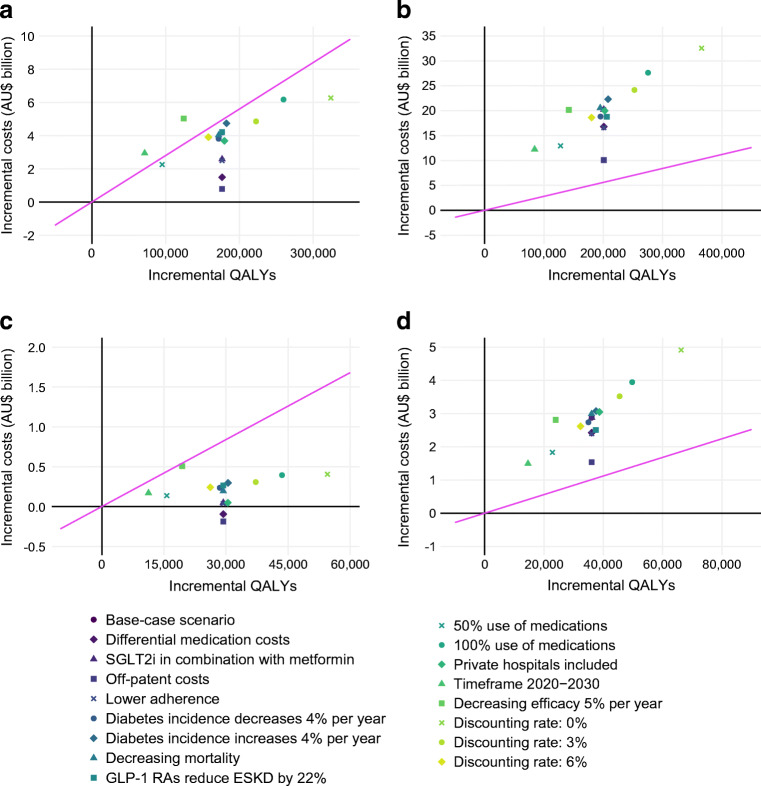
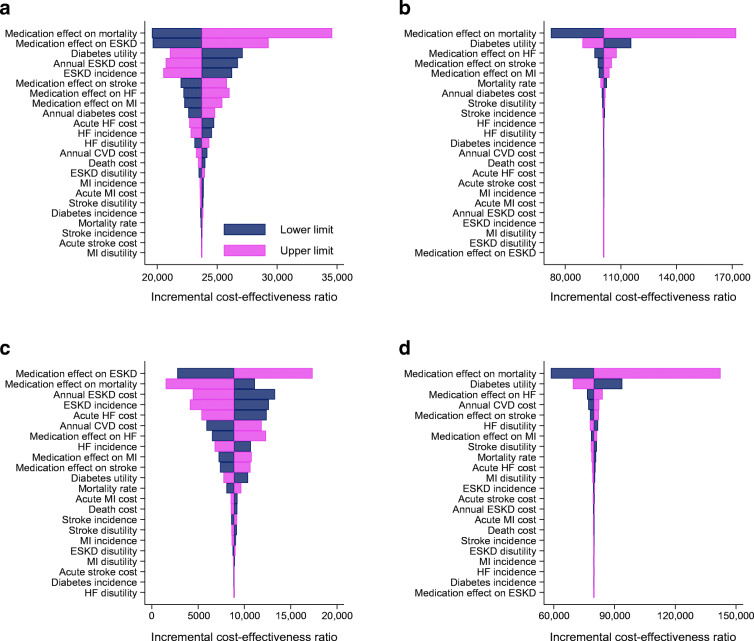
The numbers of QALYs gained from 2020 to 2040 with increased SGLT2i and GLP-1 RA use in the total population (n=1.1 million in 2020; n=1.5 million in 2040) were 176,446 and 200,932, respectively, compared with current use. Net cost differences were AU$4.2 billion for SGLT2is and AU$20.2 billion for GLP-1 RAs, and the ICERs were AU$23,717 and AU$100,705 per QALY gained, respectively. In the secondary prevention population, the ICERs were AU$8878 for SGLT2is and AU$79,742 for GLP-1 RAs.
CONCLUSIONS/INTERPRETATION: At current prices, use of SGLT2is, but not GLP-1 RAs, would be cost-effective when considering only their cardiovascular and kidney disease benefits for people with type 2 diabetes.
目的/假设:单独基于钠-葡萄糖共转运蛋白 2 抑制剂 (SGLT2is) 或胰高血糖素样肽-1 受体激动剂 (GLP-1 RAs) 的心血管和肾脏益处,它们是否具有成本效益尚不清楚。我们预测了在这些药物广泛使用的情况下,2 型糖尿病患者(有无心血管疾病)心肌梗死 (MI)、中风、心力衰竭 (HF) 和终末期肾病 (ESKD) 的健康和经济结果。
我们使用真实世界的数据设计了一个微观模拟模型,该模型捕获了 2020 年至 2040 年期间 CVD 和 ESKD 的发病率和死亡率。人群和转移概率是通过将澳大利亚糖尿病登记处(110 万 2 型糖尿病患者)与医院入院数据库、国家死亡索引和使用 2010 年至 2019 年数据的 ESKD 登记处联系起来获得的。我们模拟了四种干预措施:将 SGLT2is 或 GLP-1 RAs 的使用增加到 2 型糖尿病患者总数的 75%,以及将 SGLT2is 或 GLP-1 RAs 的使用增加到二级预防人群(即患有 2 型糖尿病和既往 CVD 的人群)的 75%。所有干预措施均与目前 SGLT2is(总人口的 20%)和 GLP-1 RAs(总人口的 5%)的使用情况进行了比较。感兴趣的结果包括质量调整生命年 (QALYs)、总费用(从澳大利亚公共医疗保健角度)和增量成本效益比 (ICER)。我们对健康经济学结果应用了 5%的年度贴现。支付意愿阈值设定为每获得一个质量调整生命年 (QALY) 支付 28000 澳元。
与当前使用相比,在 2020 年至 2040 年期间,SGLT2i 和 GLP-1 RA 在总人口中的使用(2020 年为 110 万;2040 年为 150 万)分别增加了 176,446 和 200,932 个 QALYs。净成本差异分别为 SGLT2is 为 42 亿澳元,GLP-1 RAs 为 202 亿澳元,ICER 分别为每获得一个 QALY 分别为 23,717 澳元和 100,705 澳元。在二级预防人群中,SGLT2is 的 ICER 为 8878 澳元,GLP-1 RAs 的 ICER 为 79742 澳元。
结论/解释:以目前的价格,仅考虑 SGLT2is 的心血管和肾脏疾病益处,SGLT2is 而不是 GLP-1 RAs 对 2 型糖尿病患者具有成本效益。