Department of Hepatopancreatobiliary Surgery, Chongqing General Hospital, Chongqing, China (mainland).
Department of Surgery, Hospital of People's Liberation Army Unit 63820, Mianyang, Sichuan, China (mainland).
Med Sci Monit. 2022 Nov 21;28:e938443. doi: 10.12659/MSM.938443.
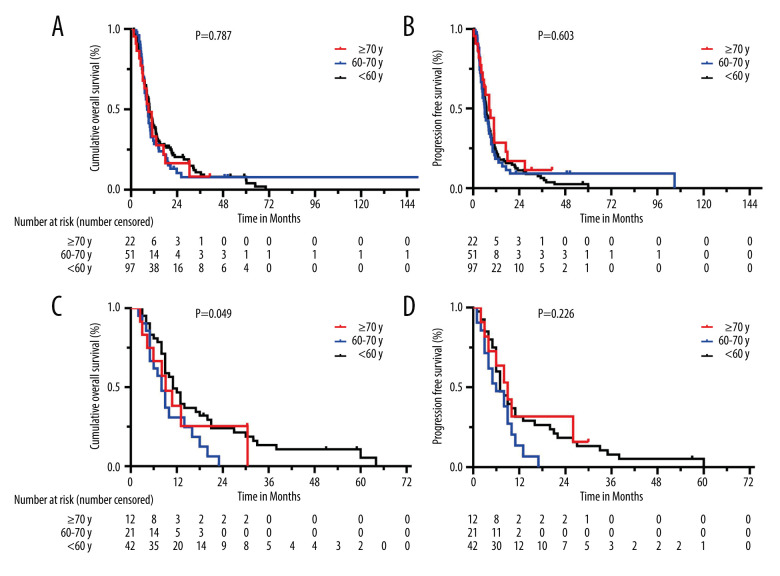
BACKGROUND Pancreaticoduodenectomy combined with revascularization (PDR) is the main surgical procedure for resectable pancreatic ductal adenocarcinoma (PDAC) with venous system invasion, but this procedure is discouraged in elderly patients because of physical complexity. Our aim was to explore the differences of perioperative and survival in patients of different ages who underwent PDR. MATERIAL AND METHODS We reviewed data from PDAC patients undergoing PDR from 2007 to 2018. Patients were subdivided into 3 groups according to age: <60 years, 60-70 years, and ≥70 years. Postoperative complications and long-term survival were compared among the 3 groups. RESULTS From 626 patients, 185 had en bloc venous resection who underwent PDR (103, 55, and 27 patients from young to elderly). Increasing age was linked to a higher prevalence of ICU management (P=0.035) and more serious complications (grade ≥III, P=0.043); overall mortality was 8.1% and did not significantly differ among age-matched groups. Further, there was no difference in overall survival (OS) or progression-free survival (PFS) based on age (<60, 60-70, ≥70, median OS were 9.7, 8.4 vs 9.1 months, respectively, P=0.787; median PFS were 6.9, 6.1 vs 8.4 months, respectively, P=0.603). However, patients <60 years whose tumors invaded the superior mesenteric vascular had better survival outcomes when compared with the other 2 groups (11.5 vs 8.4, 9.1 months, P=0.049). CONCLUSIONS The results show that age should not be considered an absolute contraindication for PDR, as elderly patients can achieve the same surgical efficacy and long-term survival prognosis.
胰十二指肠切除术联合血管重建(PDR)是可切除的胰腺导管腺癌(PDAC)伴静脉系统侵犯的主要手术方法,但由于手术复杂性,该手术在老年患者中不被鼓励。我们的目的是探讨不同年龄接受 PDR 的患者围手术期和生存差异。
我们回顾了 2007 年至 2018 年期间接受 PDR 的 PDAC 患者的数据。根据年龄将患者分为 3 组:<60 岁、60-70 岁和≥70 岁。比较 3 组患者的术后并发症和长期生存情况。
从 626 例患者中,有 185 例行整块静脉切除的 PDR 手术(年轻至老年患者分别为 103、55 和 27 例)。年龄增长与 ICU 管理(P=0.035)和更严重的并发症(≥III 级,P=0.043)的发生率较高相关;总死亡率为 8.1%,在年龄匹配组之间无显著差异。此外,根据年龄,总生存率(OS)或无进展生存率(PFS)没有差异(<60、60-70、≥70 岁,中位 OS 分别为 9.7、8.4 与 9.1 个月,P=0.787;中位 PFS 分别为 6.9、6.1 与 8.4 个月,P=0.603)。然而,与其他 2 组相比,<60 岁且肿瘤侵犯肠系膜上血管的患者生存结果更好(11.5 与 8.4、9.1 个月,P=0.049)。
结果表明,年龄不应作为 PDR 的绝对禁忌证,因为老年患者可以获得相同的手术疗效和长期生存预后。