Shi Yiming, Yang Chunhua, Chen Lei, Cheng Min, Xie Wenfeng
Intensive Care Unit, The Sixth Affiliated Hospital, Sun Yat-sen University, Guangzhou 510655, PR China.
Heliyon. 2022 Nov 16;8(11):e11498. doi: 10.1016/j.heliyon.2022.e11498. eCollection 2022 Nov.
Among critically ill patients in the intensive care unit (ICU), sepsis is an urgent global public health problem due to its high incidence, high mortality rate and complex pathogenesis.
This study was to evaluate the predictive value of neutrophil-to-lymphocyte ratio (NLR), and neutrophil-to-lymphocyte and platelet ratio (NLPR) in-hospital mortality in septic patients on days 1, 3 and 5 in ICU.
The data of septic patients admitted to the ICU of the Sixth Affiliated Hospital of Sun Yat-sen University from March, 2018 to July, 2019 were collected. NLR and NLPR were calculated and multivariate logistic regression analysis was performed to identify the relationship between them and in-hospital mortality, respectively. Receiver operating characteristic curve (ROC) was used to determine the efficacy and optimal cutoff value of diagnostic tests.
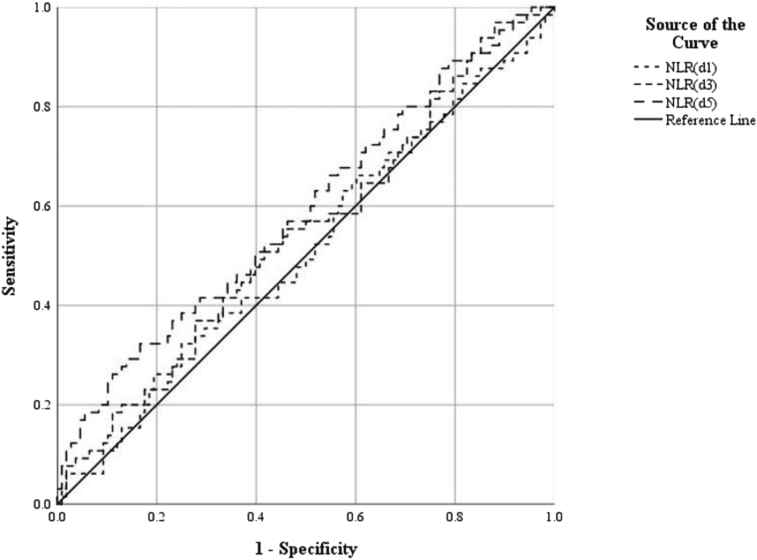
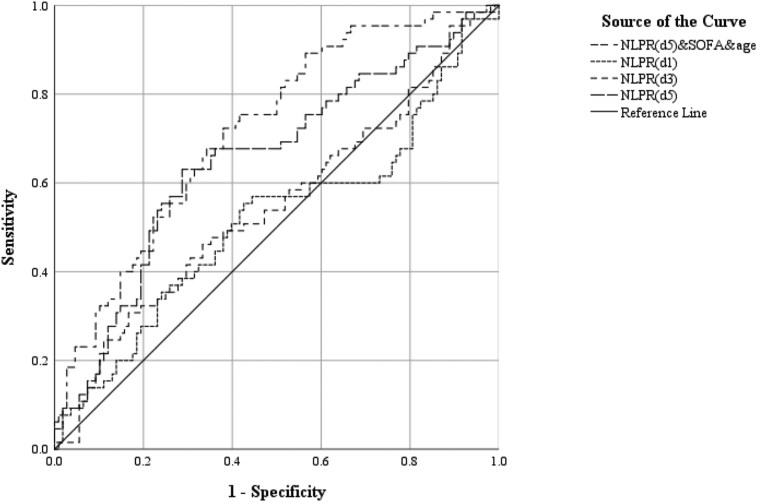
A total of 173 septic patients were included in this analysis, including 108 cases in the survival group and 65 in the death group, with a total mortality rate of 37.6%. A multivariate logistic regression analysis showed that NLR on day 5 was independently correlated with in-hospital mortality rate (OR 1.041, 95% CI: 1.008-1.074), and Day 5 NLPR was also independently associated with in-hospital mortality rate (OR 1.020, 95% CI: 1.001-1.040). The areas under the receiver operating characteristic curve (AUC) of the NLR on days 1 and 3 was 0.513 and 0.542 respectively, and the optimal cutoff value were 23.16 and 15.48, and the AUC of the NLR on day 5 was 0.589, and the best cutoff value was 15.85. The AUC of NLPR on day 1 and 3 was 0.517 and 0.547, respectively, and the optimal cutoff value was 10.25 and 18.47. The AUC of NLPR on day 5 was the largest, 0.654, and the optimal cutoff value was 8.22. After combined NLPR on day 5 with age and sequential organ failure assessment (SOFA) scores, the AUC increase to 0.718. Among the joint predictors, the optimal cutoff value for NLPR on day 5 was 9.31.
We found that Day 5 NLPR and NLR were independently correlated with in-hospital mortality. Day 5 NLPR Combined with age and SOFA scores may be help predict mortality in ICU septic hospitalized patients.
在重症监护病房(ICU)的重症患者中,脓毒症因其高发病率、高死亡率和复杂的发病机制,是一个紧迫的全球公共卫生问题。
本研究旨在评估中性粒细胞与淋巴细胞比值(NLR)以及中性粒细胞与淋巴细胞和血小板比值(NLPR)对ICU中脓毒症患者第1、3和5天院内死亡率的预测价值。
收集2018年3月至2019年7月在中山大学附属第六医院ICU住院的脓毒症患者的数据。计算NLR和NLPR,并分别进行多因素逻辑回归分析以确定它们与院内死亡率之间的关系。采用受试者工作特征曲线(ROC)来确定诊断试验的效能和最佳截断值。
本分析共纳入173例脓毒症患者,其中存活组108例,死亡组65例,总死亡率为37.6%。多因素逻辑回归分析显示,第5天的NLR与院内死亡率独立相关(OR 1.041,95%CI:1.008 - 1.074),第5天的NLPR也与院内死亡率独立相关(OR 1.020,95%CI:1.001 - 1.040)。第1天和第3天NLR的受试者工作特征曲线(AUC)下面积分别为0.513和0.542,最佳截断值分别为23.16和15.48,第5天NLR的AUC为0.589,最佳截断值为15.85。第1天和第3天NLPR的AUC分别为0.517和0.547,最佳截断值为10.25和18.47。第5天NLPR的AUC最大,为0.654,最佳截断值为8.22。将第5天的NLPR与年龄和序贯器官衰竭评估(SOFA)评分联合后,AUC增至0.718。在联合预测指标中,第5天NLPR的最佳截断值为9.31。
我们发现第5天的NLPR和NLR与院内死亡率独立相关。第5天的NLPR联合年龄和SOFA评分可能有助于预测ICU脓毒症住院患者的死亡率。