Hafeez Shaista, Koh Mu, Jones Kelly, Ghzal Amir El, D'Arcy James, Kumar Pardeep, Khoo Vincent, Lalondrelle Susan, McDonald Fiona, Thompson Alan, Scurr Erica, Sohaib Aslam, Huddart Robert Anthony
Division of Radiotherapy and Imaging, The Institute of Cancer Research, London, United Kingdom.
Urology Unit, The Royal Marsden National Health Service (NHS) Foundation Trust, London, United Kingdom.
Front Oncol. 2022 Nov 14;12:961393. doi: 10.3389/fonc.2022.961393. eCollection 2022.
This study aims to determine local treatment response and long-term survival outcomes in patients with localised muscle-invasive bladder cancer (MIBC) patients receiving neoadjuvant chemotherapy (NAC) using diffusion-weighted MRI (DWI) and apparent diffusion coefficient (ADC) analysis.
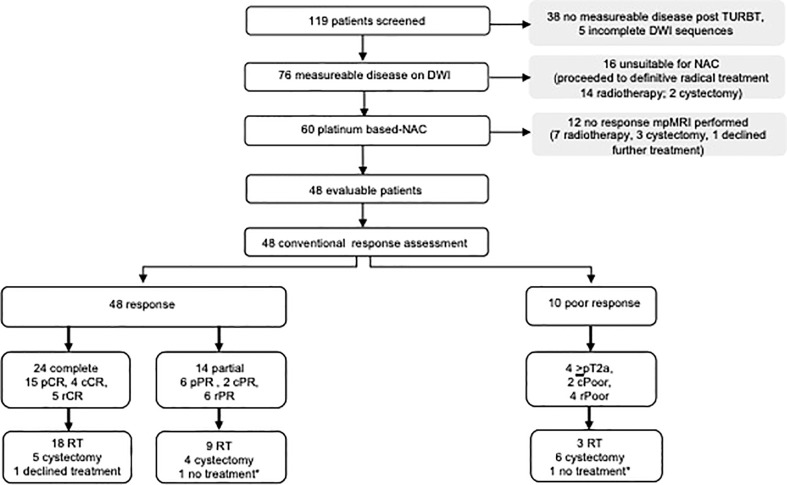
Patients with T2-T4aN0-3M0 bladder cancer suitable for NAC were recruited prospectively. DWI was performed prior to NAC and was repeated following NAC completion. Conventional response assessment was performed with cystoscopy and tumour site biopsy. Response was dichotomised into response (<T2) or poor response (≥T2). Patients proceeded to either radical cystectomy or chemo-radiotherapy as standard of care. Tumour ADC values were calculated for all b-values (ADC) and high b-values (ADC). Mean ADC, percentiles, skew, kurtosis, and their change (ΔADC and %ΔADC) were determined. Threshold predictive of response with highest specificity was ascertained using receiver operating characteristic (ROC) analysis. Median overall survival (OS), bladder-cancer-specific survival (bCSS), progression-free survival (PFS), and time to cystectomy were estimated using Kaplan-Meier method. Significant area under the curve (AUC) cut points were used to determine relationship with long-term endpoints and were compared using log-rank test.
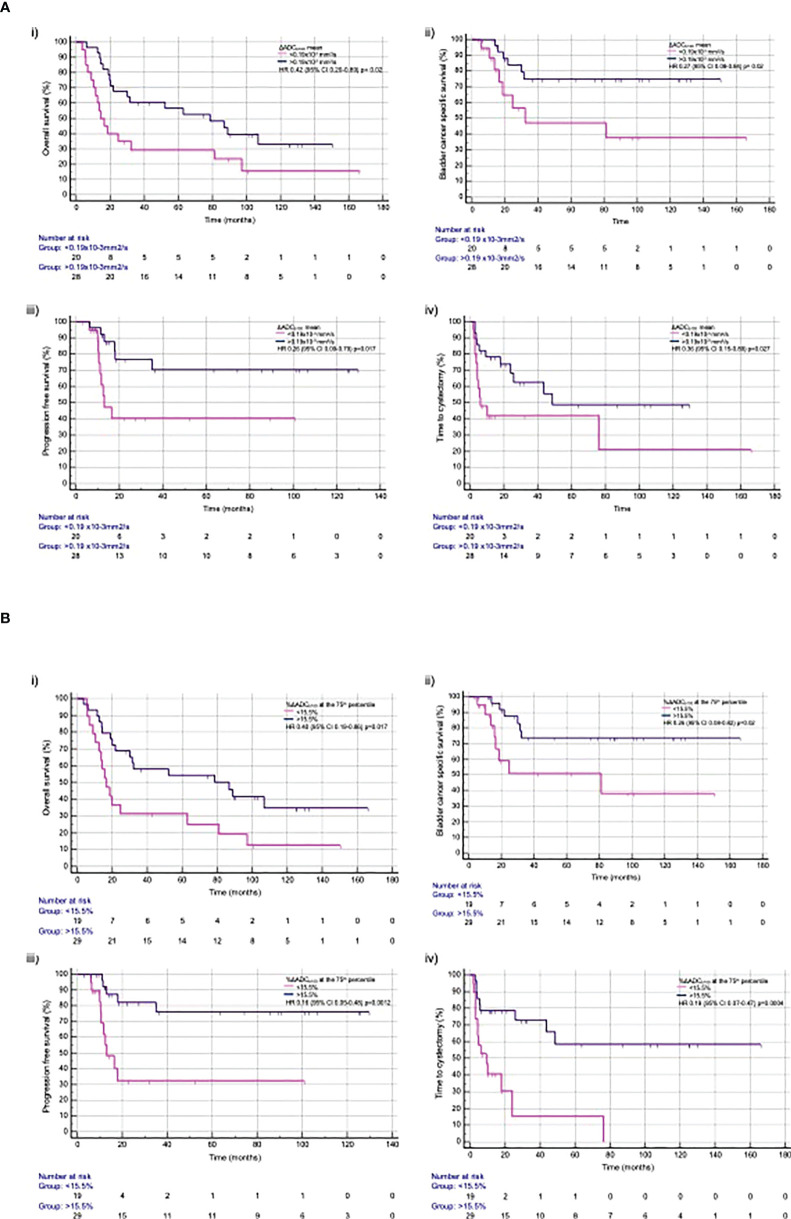
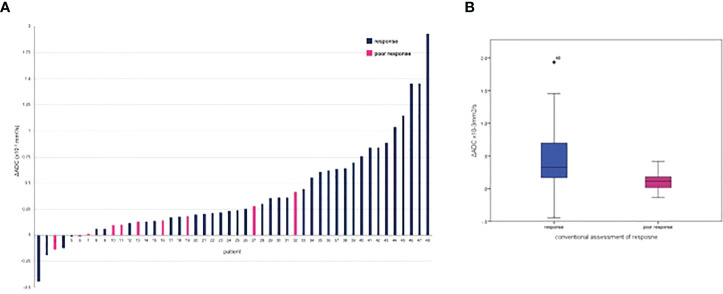
Forty-eight patients (96 DWI) were evaluated. NAC response was associated with significant increase in mean ΔADC and %ΔADC compared to poor response (ΔADC 0.32×10 versus 0.11×10 mm/s; p=0.009, and %ΔADC 21.70% versus 8.23%; p=0.013). Highest specificity predicting response was seen at 75th percentile ADC (AUC, 0.8; p=0.01). Sensitivity, specificity, positive predictive power, and negative predictive power of %ΔADC 75th percentile was 73.7%, 90.0%, 96.6%, and 52.9%, respectively. %ΔADC 75th percentile >15.5% was associated with significant improvement in OS (HR, 0.40; 95% CI, 0.19-0.86; p=0.0179), bCSS (HR, 0.26; 95% CI, 0.08-0.82; p=0.0214), PFS (HR, 0.16; 95% CI, 0.05-0.48; p=0.0012), and time to cystectomy (HR, 0.19; 95% CI, 0.07-0.47; p=0.0004).
Quantitative ADC analysis can successfully identify NAC response and improved long-term clinical outcomes. Multi-centre validation to assess reproducibility and repeatability is required before testing within clinical trials to inform MIBC treatment decision making.
We successfully demonstrated that measured change in DWI can successfully identify NAC response and improved long-term survival outcomes.
本研究旨在通过扩散加权磁共振成像(DWI)和表观扩散系数(ADC)分析,确定接受新辅助化疗(NAC)的局限性肌肉浸润性膀胱癌(MIBC)患者的局部治疗反应和长期生存结果。
前瞻性招募适合NAC的T2-T4aN0-3M0膀胱癌患者。在NAC之前进行DWI,并在NAC完成后重复进行。通过膀胱镜检查和肿瘤部位活检进行传统的反应评估。反应分为反应(<T2)或反应不佳(≥T2)。患者按照标准治疗进行根治性膀胱切除术或放化疗。计算所有b值(ADC)和高b值(ADC)的肿瘤ADC值。确定平均ADC、百分位数、偏度、峰度及其变化(ΔADC和%ΔADC)。使用受试者工作特征(ROC)分析确定具有最高特异性的反应预测阈值。使用Kaplan-Meier方法估计中位总生存期(OS)、膀胱癌特异性生存期(bCSS)、无进展生存期(PFS)和膀胱切除时间。使用曲线下显著面积(AUC)切点确定与长期终点的关系,并使用对数秩检验进行比较。
评估了48例患者(96次DWI)。与反应不佳相比,NAC反应与平均ΔADC和%ΔADC的显著增加相关(ΔADC 0.32×10对0.11×10 mm²/s;p=0.009,%ΔADC 21.70%对8.23%;p=0.013)。在第75百分位ADC处观察到预测反应的最高特异性(AUC,0.8;p=0.01)。第75百分位%ΔADC的敏感性、特异性、阳性预测能力和阴性预测能力分别为73.7%、90.0%、96.6%和52.9%。第75百分位%ΔADC>15.5%与OS(HR,0.40;95%CI,0.19-0.86;p=0.0179)、bCSS(HR,0.26;95%CI,0.08-0.82;p=0.0214)、PFS(HR,0.16;95%CI,0.05-0.48;p=0.0012)和膀胱切除时间(HR,0.19;95%CI,0.07-0.47;p=0.0004)的显著改善相关。
定量ADC分析可以成功识别NAC反应并改善长期临床结果。在临床试验中进行测试以指导MIBC治疗决策之前,需要进行多中心验证以评估可重复性和再现性。
我们成功证明,DWI测量的变化可以成功识别NAC反应并改善长期生存结果。