Abramson Cancer Center, University of Pennsylvania, Philadelphia, Pennsylvania.
Winship Cancer Institute, Hematology and Medical Oncology, Emory University School of Medicine, Atlanta, Georgia.
Clin Cancer Res. 2023 Feb 1;29(3):560-570. doi: 10.1158/1078-0432.CCR-22-1987.
Tumoral programmed cell death ligand-1 (PD-L1) expression is common in human papillomavirus (HPV)-associated head and neck squamous cell carcinoma (HNSCC). We assessed whether a DNA vaccine targeting HPV-16/18 E6/E7 with IL12 adjuvant (MEDI0457) combined with the PD-L1 inhibitor durvalumab could enhance HPV-specific T-cell response and improve outcomes in recurrent/metastatic HPV-16/18-associated HNSCC.
In this phase Ib/IIa study, immunotherapy-naïve patients with ≥1 previous platinum-containing regimen (neoadjuvant/adjuvant therapy or for recurrent/metastatic disease) received MEDI0457 7 mg intramuscularly with electroporation on weeks 1, 3, 7, and 12, then every 8 weeks, plus durvalumab 1,500 mg intravenously on weeks 4, 8, and 12, then every 4 weeks, until confirmed progression and/or unacceptable toxicity. Coprimary objectives were safety and objective response rate (ORR; H0: ORR ≤ 15%); secondary objectives included 16-week disease control rate (DCR-16), overall survival (OS), and progression-free survival (PFS).
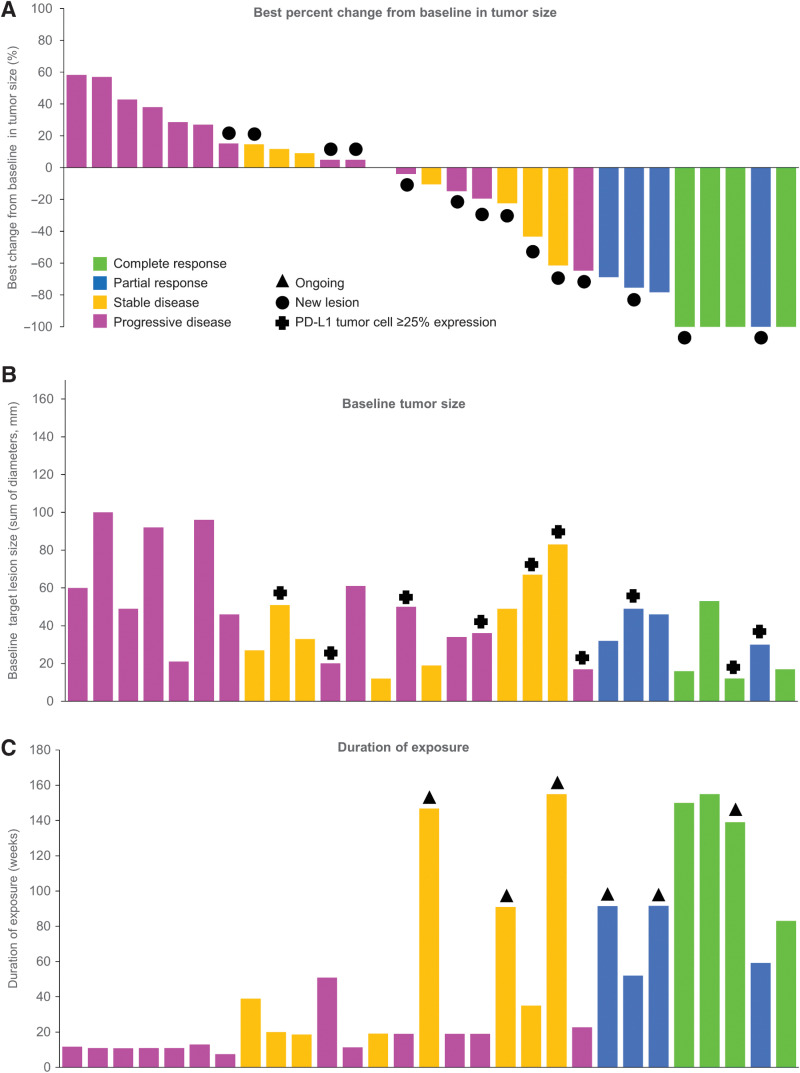
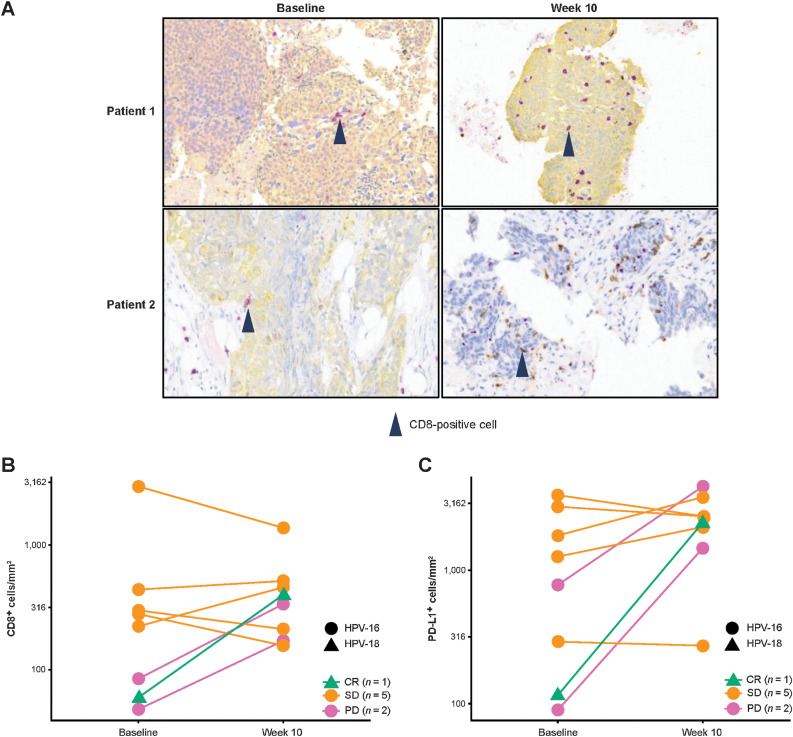
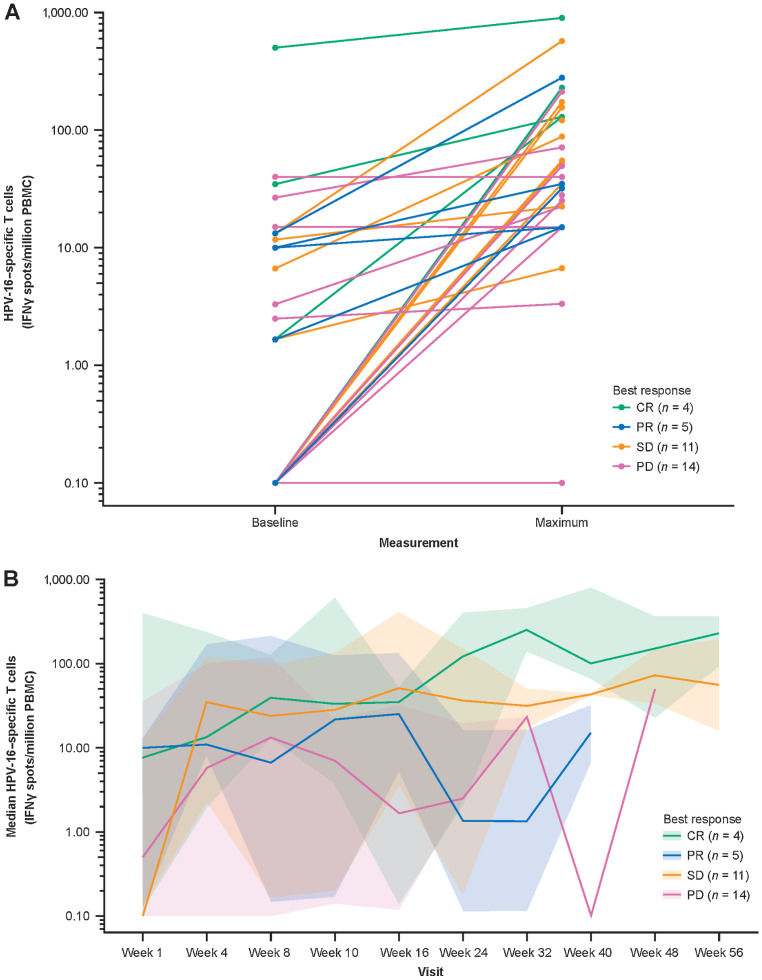
Of 35 treated patients, 29 were response evaluable (confirmed HPV-associated disease; received both agents). ORR was 27.6% [95% confidence interval (CI), 12.7-47.2; four complete responses, four partial responses]; responses were independent of PD-L1 tumor-cell expression (≥25% vs. <25%). DCR-16 was 44.8% (95% CI, 26.5-64.3). Median PFS was 3.5 months (95% CI, 1.9-9.0); median OS was 29.2 months (15.2-not calculable). Twenty-eight (80.0%) patients had treatment-related adverse events [grade 3: 5 (14.3%); no grade 4/5], resulting in discontinuation in 2 (5.7%) patients. HPV-16/18-specific T cells increased on treatment; 4 of 8 evaluable patients had a >2-fold increase in tumor-infiltrating CD8+ T cells.
MEDI0457 plus durvalumab was well tolerated. While the primary efficacy endpoint was not reached, clinical benefit was encouraging.
肿瘤程序性细胞死亡配体 1(PD-L1)在人乳头瘤病毒(HPV)相关头颈部鳞状细胞癌(HNSCC)中较为常见。我们评估了 HPV-16/18 E6/E7 靶向 DNA 疫苗与 IL12 佐剂(MEDI0457)联合 PD-L1 抑制剂 durvalumab 是否可以增强 HPV 特异性 T 细胞反应,并改善复发性/转移性 HPV-16/18 相关 HNSCC 的预后。
在这项 Ib/IIa 期研究中,接受过≥1 种含铂方案(新辅助/辅助治疗或复发性/转移性疾病)的免疫治疗初治患者接受 MEDI0457 7mg 肌内注射,联合电穿孔,在第 1、3、7 和 12 周,然后每 8 周一次,联合 durvalumab 1500mg 静脉输注,在第 4、8 和 12 周,然后每 4 周一次,直至确认疾病进展和/或不可接受的毒性。主要研究目的是安全性和客观缓解率(ORR;H0:ORR≤15%);次要研究目的包括 16 周疾病控制率(DCR-16)、总生存期(OS)和无进展生存期(PFS)。
在 35 例接受治疗的患者中,有 29 例(确认 HPV 相关疾病;接受两种药物治疗)可评估反应。ORR 为 27.6%(95%CI,12.7-47.2;4 例完全缓解,4 例部分缓解);反应与 PD-L1 肿瘤细胞表达无关(≥25%与<25%)。DCR-16 为 44.8%(95%CI,26.5-64.3)。中位 PFS 为 3.5 个月(95%CI,1.9-9.0);中位 OS 为 29.2 个月(15.2-未计算)。28 例(80.0%)患者发生治疗相关不良事件(3 级:5 例[14.3%];无 4/5 级),2 例(5.7%)患者因不良事件停药。治疗期间 HPV-16/18 特异性 T 细胞增加;8 例可评估患者中有 4 例肿瘤浸润 CD8+T 细胞增加了>2 倍。
MEDI0457 联合 durvalumab 耐受性良好。虽然主要疗效终点未达到,但临床获益令人鼓舞。