Department of Sports Medicine, Beijing Ji Shui Tan Hospital, 4th Affiliated Hospital of Peking University, Beijing, China.
Orthop Surg. 2023 Aug;15(8):1967-1974. doi: 10.1111/os.13534. Epub 2022 Dec 2.
There was no universally accepted classification system that describes LHBT lesions as a type of its' pathology in patients with shoulder pain. This study aimed to determine the correlation of anatomic variants of glenoid labrum attachment of long head of biceps tendon (LHBT) and to assess their association, if any, with its lesions in rotator cuff tear (RCT) patients.
All RCT patients from January 2016 to December 2019 were assessed arthroscopically to classify the LHBT labrum attachment according to its' anatomical location. A simplified classification was created to describe the LHBT as normal, tendinitis, subluxation or dislocation, partial tear and superior labral tear from anterior to posterior (SLAP) lesion beyond type II The RCT were classified as three types as partial, small to medium and large to massive. The correlation of variants of LHBT labral attachment with type of LHBT lesions in different RCT groups was evaluated.
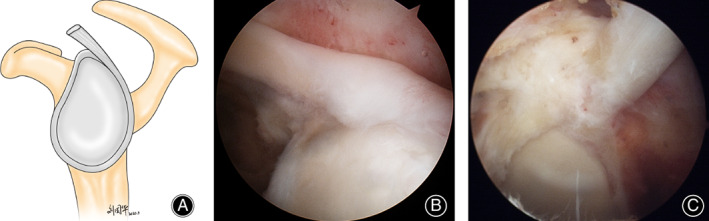
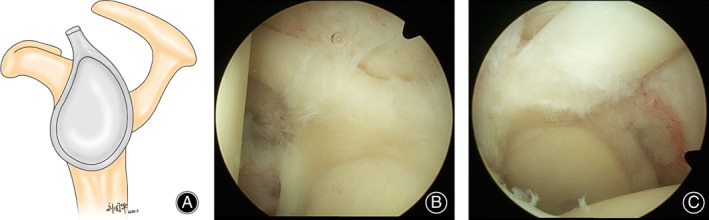
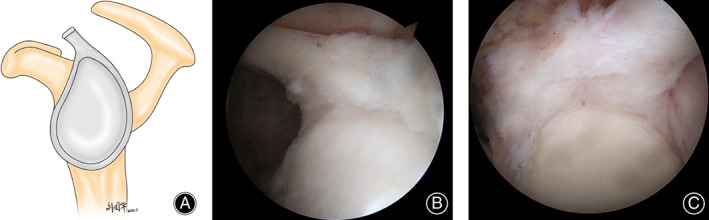
In total, 669 patients were included for evaluation. The attachment of the LHBT was entirely posterior in 23 shoulders (3.4%), posterior-dominant in 81 shoulders (12.1%), and equal in 565 shoulders (84.4%). In equal distribution LHBT attachment group, age > 60 (odds ratio: 2.928, P < 0.001) and size of RCT (P < 0.001) were significant risk factors of LHBT lesions. In the analysis of all patients, comparing with the partial thickness rotator cuff tear (PTRCT), the odds ratio of small to medium RCT and large to massive RCT was 2.398 and 6.606 respectively. In addition, age > 60 (odds ratio: 2.854, P < 0.001) and size of RCT (P < 0.001) were significant risk factors of LHBT lesions. In posterior dominant group, size of RCT was a significant risk factor of LHBT lesions but not any others (P < 0.001). In entirely posterior group, no risk factor of LHBT lesions was found. It showed that the variation of LHBT attachment was not a significant risk factor of LHBT lesions in rotator cuff repaired patients (p = 0.075).
There are three types of LHBT labrum attachment in RCT patients on arthroscopic observation. 84.4% were equal distribution of LHBT attachment on glenoid labrum, followed by posterior-dominant (12.1%) and entirely posterior type (3.4%) in present study. Although the variation of LHBT attachment was not a significant risk factor of LHBT lesion in rotator cuff repaired(RCR) patients, there were different risk factors among three LHBT labral attachment types. In RCR patients, age > 60 and RCT size were significant risk factors of LHBT lesions.
目前尚没有一个通用的分类系统能够将肩痛患者的长头肱二头肌肌腱(LHBT)的 LHBT 病变描述为其病理学的一种类型。本研究旨在确定盂唇附着处 LHBT 解剖变异与肩袖撕裂(RCT)患者 LHBT 病变之间的相关性,并评估其任何相关性。
对 2016 年 1 月至 2019 年 12 月所有 RCT 患者进行关节镜评估,根据其解剖位置对 LHBT 盂唇附着处进行分类。创建了一种简化分类方法,将 LHBT 描述为正常、肌腱炎、半脱位或脱位、部分撕裂和从前到后(SLAP)的 Superior 盂唇撕裂(Ⅱ型以上)病变。将 RCT 分为三种类型:部分撕裂、小到中等撕裂和大到巨大撕裂。评估不同 RCT 组中 LHBT 盂唇附着处的变异与 LHBT 病变类型之间的相关性。
共纳入 669 例患者进行评估。LHBT 的附着在 23 例(3.4%)中完全位于后部,81 例(12.1%)中后部占主导地位,565 例(84.4%)中相等。在 LHBT 附着均匀分布组中,年龄>60 岁(优势比:2.928,P<0.001)和 RCT 大小(P<0.001)是 LHBT 病变的显著危险因素。在所有患者的分析中,与部分厚度肩袖撕裂(PTRCT)相比,小到中等 RCT 和大到巨大 RCT 的比值比分别为 2.398 和 6.606。此外,年龄>60 岁(优势比:2.854,P<0.001)和 RCT 大小(P<0.001)是 LHBT 病变的显著危险因素。在后主导组中,RCT 大小是 LHBT 病变的显著危险因素,但不是其他任何因素(P<0.001)。在完全后部组中,未发现 LHBT 病变的危险因素。这表明在肩袖修复患者中,LHBT 附着的变化不是 LHBT 病变的显著危险因素(p=0.075)。
在关节镜观察下,RCT 患者有三种类型的 LHBT 盂唇附着。本研究中,84.4%的 LHBT 附着在盂唇上呈均匀分布,其次是后主导型(12.1%)和完全后部型(3.4%)。尽管在肩袖修复(RCR)患者中,LHBT 附着的变化不是 LHBT 病变的显著危险因素,但在三种 LHBT 盂唇附着类型中存在不同的危险因素。在 RCR 患者中,年龄>60 岁和 RCT 大小是 LHBT 病变的显著危险因素。