Department of Geriatrics, Zhejiang Hospital, Hangzhou, Zhejiang, People's Republic of China.
Clin Interv Aging. 2022 Nov 29;17:1697-1706. doi: 10.2147/CIA.S376691. eCollection 2022.
This study aimed to investigate the combined effects of frailty and cognitive impairment on adverse outcomes, including new falls and new activities of daily living (ADL) dependency over a 1-year follow-up.
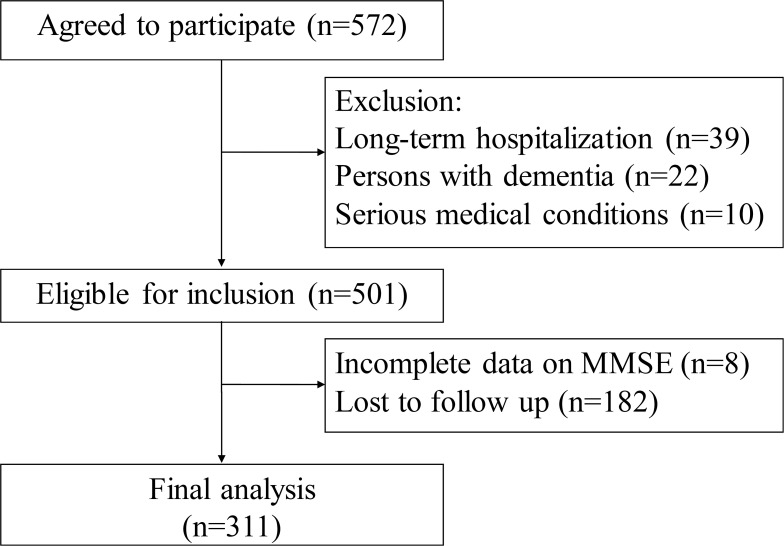
A total of 311 older hospitalized patients participated in this retrospective observational study and completed a 1-year follow-up. Frailty was assessed by the Clinical Frailty Scale (CFS). Cognitive function was evaluated by the Mini-Mental State Examination (MMSE). All participants were classified into four groups: 1) the healthy group (n=180); 2) the cognitive impairment group only (n=38); 3) the frailty group only (n=44); and 4) coexisting frailty and cognitive impairment group (n=49). The follow-up data of adverse outcomes include the incidences of new falls and new ADL dependence. Binary logistic regression analysis was used to explore the associations of frailty and/or cognitive impairment with adverse outcomes.
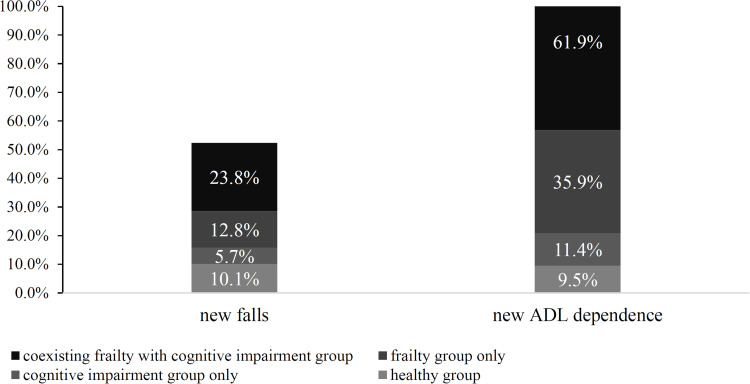
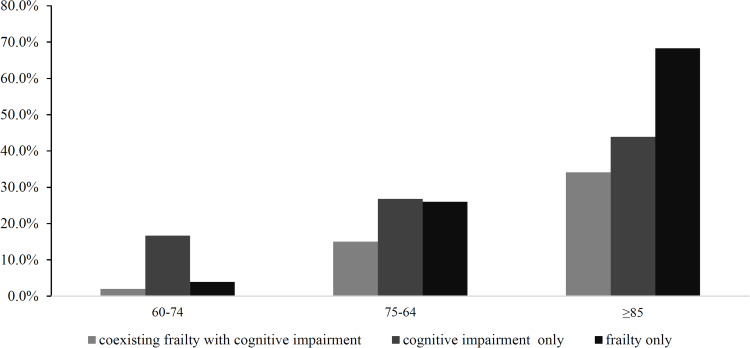
The prevalence rates of frailty, cognitive impairment, and co-occurring frailty with cognitive impairment were 29.9%, 28%, and 15.8%, respectively. Among these four groups, there was a statistical difference in the incidence of new ADL dependence during the follow-up period (9.5% vs 11.4% vs 35.9% vs 61.9%, < 0.001). After adjusting the confounding variables, older hospitalized patients with frailty and cognitive impairment had a higher risk of new ADL dependence when compared with the healthy group (OR: 4.786, 95% CI: 1.492-15.355), but frailty only or cognitive impairment only was not associated with new ADL dependency.
Elderly inpatients with comorbid frailty and cognitive impairment on admission were significantly associated with an increased risk of new ADL dependency 1 year after discharge. Therefore, it is necessary for the early identification of frailty and cognitive impairment, and effective interventions should be implemented.
本研究旨在探讨衰弱和认知障碍对不良结局的综合影响,包括在 1 年随访期间新的跌倒和新的日常生活活动(ADL)依赖。
共有 311 名老年住院患者参与了这项回顾性观察研究,并完成了 1 年的随访。衰弱通过临床虚弱量表(CFS)评估。认知功能通过简易精神状态检查(MMSE)评估。所有参与者被分为四组:1)健康组(n=180);2)仅认知障碍组(n=38);3)仅衰弱组(n=44);4)衰弱和认知障碍共存组(n=49)。不良结局的随访数据包括新跌倒和新 ADL 依赖的发生率。使用二项逻辑回归分析探讨衰弱和/或认知障碍与不良结局的关系。
衰弱、认知障碍和衰弱与认知障碍共存的患病率分别为 29.9%、28%和 15.8%。在这四组中,在随访期间新的 ADL 依赖发生率存在统计学差异(9.5%比 11.4%比 35.9%比 61.9%,<0.001)。在调整混杂变量后,与健康组相比,入院时患有衰弱和认知障碍的老年住院患者发生新的 ADL 依赖的风险更高(OR:4.786,95%CI:1.492-15.355),但衰弱或认知障碍本身与新的 ADL 依赖无关。
入院时患有衰弱和认知障碍共存的老年住院患者 1 年后发生新的 ADL 依赖的风险显著增加。因此,有必要早期识别衰弱和认知障碍,并实施有效的干预措施。