Pharmacy Practice Department, Cedarville University School of Pharmacy, Cedarville, Ohio, USA.
Miami Valley Hospital, Dayton, Ohio, USA.
Pharmacotherapy. 2023 Jan;43(1):53-84. doi: 10.1002/phar.2748. Epub 2022 Dec 20.
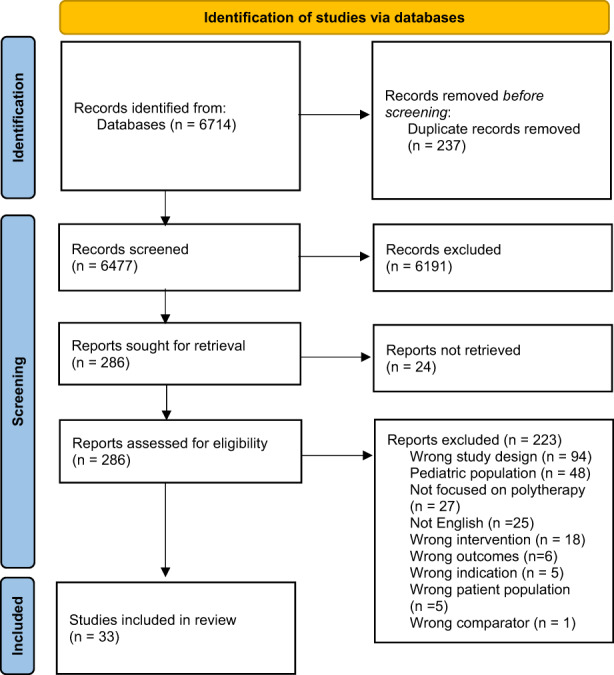
There is a paucity of literature regarding the optimal selection of combination antiseizure medications (ASMs) for drug-resistant epilepsy (DRE). The aim of this scoping review is to evaluate current evidence related to "rational polytherapy" among adults with DRE. Using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews (PRISMA-SCr) guidelines, PubMed, ProQuest, CINAHL, and Cochrane databases were searched using DRE- and polytherapy-related keywords. The exclusion criteria applied included: non-English; non-human studies; non-research studies; participants less than 18 years; status epilepticus; ASM monotherapy; and certain ASMs. In Covidence, two researchers independently reviewed articles for inclusion at each phase, with a third resolving conflicts. Data were extracted, with quality appraisal using the Mixed Methods Appraisal Tool (MMAT). Of the 6477 studies imported for screening, 33 studies were included. Clinical, humanistic, and economic outcomes were reported by 26, 12, and one study, respectively. Common efficacy-related clinical outcomes included ≥50% reduction in seizure frequency (n = 14), seizure freedom (n = 14), and percent reduction in seizure frequency (n = 8). Common humanistic outcomes included quality of life (n = 4), medication adherence (n = 2), sleep-related outcomes (n = 2), and physician and patient global assessments (n = 2). The economic study reported quality-adjusted life years. The median MMAT score was 80 (range: 60-100). Two studies referenced the standard definition of DRE, whereas five studies did not specifically define DRE. Gaps in the literature include limited generalizability, minimal reports in pregnancy, and lack of optimal ASM combinations, among others. Strengths of the evidence include addressing a variety of outcomes. Inconsistent definitions of DRE, small sample sizes, and heterogeneity among studies limit the ability to draw meaningful conclusions. Optimal combinations of ASMs for rational polytherapy for DRE is unclear.
关于耐药性癫痫 (DRE) 的最佳联合抗癫痫药物 (ASM) 选择,文献相对较少。本综述的目的是评估成人 DRE 中“合理的多药治疗”的现有证据。使用系统评价和荟萃分析的首选报告项目 (PRISMA-SCr) 指南,使用 DRE 和多药治疗相关关键词在 PubMed、ProQuest、CINAHL 和 Cochrane 数据库中进行搜索。排除标准包括:非英语;非人类研究;非研究研究;参与者年龄小于 18 岁;癫痫持续状态;ASM 单药治疗;和某些 ASM。在 Covidence 中,两名研究人员在每个阶段独立审查纳入的文章,第三名研究人员解决冲突。提取数据,并使用混合方法评估工具 (MMAT) 进行质量评估。在筛选出的 6477 项研究中,有 33 项研究被纳入。分别有 26、12 和 1 项研究报告了临床、人文和经济结果。常见的与疗效相关的临床结果包括癫痫发作频率减少≥50%(n=14)、无癫痫发作(n=14)和癫痫发作频率减少百分比(n=8)。常见的人文结果包括生活质量(n=4)、药物依从性(n=2)、睡眠相关结果(n=2)和医生和患者总体评估(n=2)。经济研究报告了质量调整生命年。MMAT 评分中位数为 80(范围:60-100)。两项研究参考了 DRE 的标准定义,而五项研究未明确定义 DRE。文献中的空白包括可推广性有限、妊娠报告很少以及缺乏最佳 ASM 组合等。证据的优势包括解决了各种结果。DRE 的定义不一致、样本量小以及研究之间的异质性限制了得出有意义结论的能力。DRE 合理多药治疗的最佳 ASM 组合尚不清楚。