Sveinsson Olafur, Andersson Tomas, Mattsson Peter, Carlsson Sofia, Tomson Torbjörn
From the Department of Neurology (O.S., T.T.), Karolinska University Hospital; Department of Clinical Neuroscience (O.S., T.T.) and Institute of Environmental Medicine (T.A., S.C.), Karolinska Institutet, Stockholm; Center for Occupational and Environmental Medicine (T.A.), Stockholm County Council; and Department of Neuroscience (P.M.), University of Uppsala, Sweden.
Neurology. 2020 Nov 3;95(18):e2509-e2518. doi: 10.1212/WNL.0000000000010874. Epub 2020 Sep 23.
We conducted a nationwide case-control study in Sweden to test the hypothesis that antiepileptic drugs (AEDs) mono- or polytherapy, adherence, antidepressants, neuroleptics, β-blockers, and statins are associated with sudden unexpected death in epilepsy (SUDEP) risk.
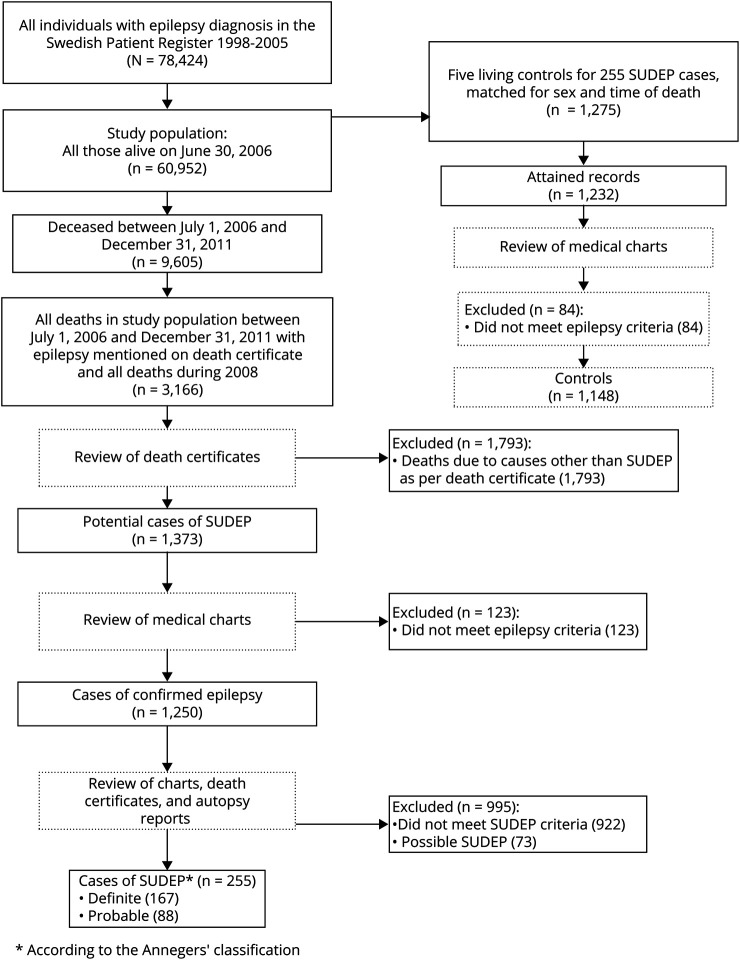
Included were 255 SUDEP cases and 1,148 matched controls. Information on clinical factors and medications came from medical records and the National Patient and Prescription Registers. The association between SUDEP and medications was assessed by odds ratios (ORs) with 95% confidence intervals (CIs) adjusted for potential risk factors including type of epilepsy, living conditions, comorbidity, and frequency of generalized tonic-clonic seizures (GTCS).
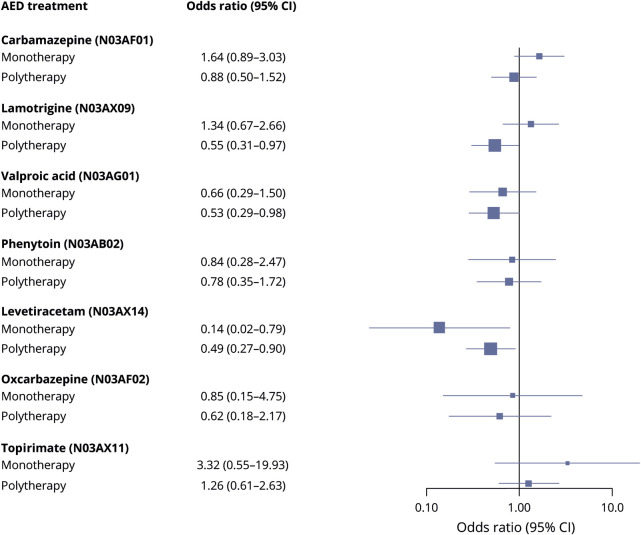
Polytherapy, especially taking 3 or more AEDs, was associated with a substantially reduced risk of SUDEP (OR 0.31, 95% CI 0.14-0.67). Combinations including lamotrigine (OR 0.55, 95% CI 0.31-0.97), valproic acid (OR 0.53, 95% CI 0.29-0.98), and levetiracetam (OR 0.49, 95% CI 0.27-0.90) were associated with reduced risk. No specific AED was associated with increased risk. Regarding monotherapy, although numbers were limited, the lowest SUDEP risk was seen in users of levetiracetam (0.10, 95% CI 0.02-0.61). Having nonadherence mentioned in the medical record was associated with an OR of 2.75 (95% CI 1.58-4.78). Statin use was associated with a reduced SUDEP risk (OR 0.34, 95% CI 0.11-0.99) but selective serotonin reuptake inhibitor use was not.
These results provide support for the importance of medication adherence and intensified AED treatment for patients with poorly controlled GTCS in the effort to reduce SUDEP risk and suggest that comedication with statins may reduce risk.
我们在瑞典开展了一项全国性病例对照研究,以检验以下假设:抗癫痫药物(AEDs)单药治疗或联合治疗、依从性、抗抑郁药、抗精神病药、β受体阻滞剂和他汀类药物与癫痫性猝死(SUDEP)风险相关。
纳入255例SUDEP病例和1148例匹配对照。临床因素和用药信息来自病历以及国家患者和处方登记处。通过优势比(ORs)及95%置信区间(CIs)评估SUDEP与药物之间的关联,并对包括癫痫类型、生活条件、合并症以及全面强直阵挛发作(GTCS)频率等潜在风险因素进行校正。
联合治疗,尤其是服用3种或更多AEDs,与SUDEP风险显著降低相关(OR 0.31,95%CI 0.14 - 0.67)。包括拉莫三嗪(OR 0.55,95%CI 0.31 - 0.97)、丙戊酸(OR 0.53,95%CI 0.29 - 0.98)和左乙拉西坦(OR 0.49,95%CI 0.27 - 0.90)的联合用药与风险降低相关。没有特定的AED与风险增加相关。关于单药治疗,尽管数量有限,但左乙拉西坦使用者的SUDEP风险最低(0.10,95%CI 0.02 - 0.61)。病历中提及不依从与OR值为2.75(95%CI 1.58 - 4.78)相关。使用他汀类药物与SUDEP风险降低相关(OR 0.34,95%CI 0.11 - 0.99),但使用选择性5-羟色胺再摄取抑制剂则不然。
这些结果支持了药物依从性以及对GTCS控制不佳的患者强化AED治疗在降低SUDEP风险方面的重要性,并表明与他汀类药物联合用药可能降低风险。