Department of Critical Care, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands.
Department of Pulmonary Medicine, Amphia Hospital, Breda, The Netherlands.
Int J Obes (Lond). 2023 Feb;47(2):126-137. doi: 10.1038/s41366-022-01246-5. Epub 2022 Dec 12.
Obesity is a risk factor for adverse outcomes in COVID-19, potentially driven by chronic inflammatory state due to dysregulated secretion of adipokines and cytokines. We investigated the association between plasma adipokines and COVID-19 severity, systemic inflammation, clinical parameters, and outcome of COVID-19 patients.
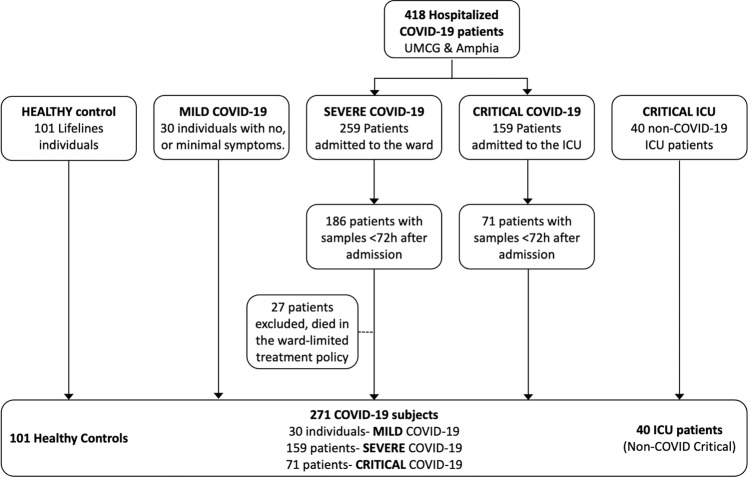
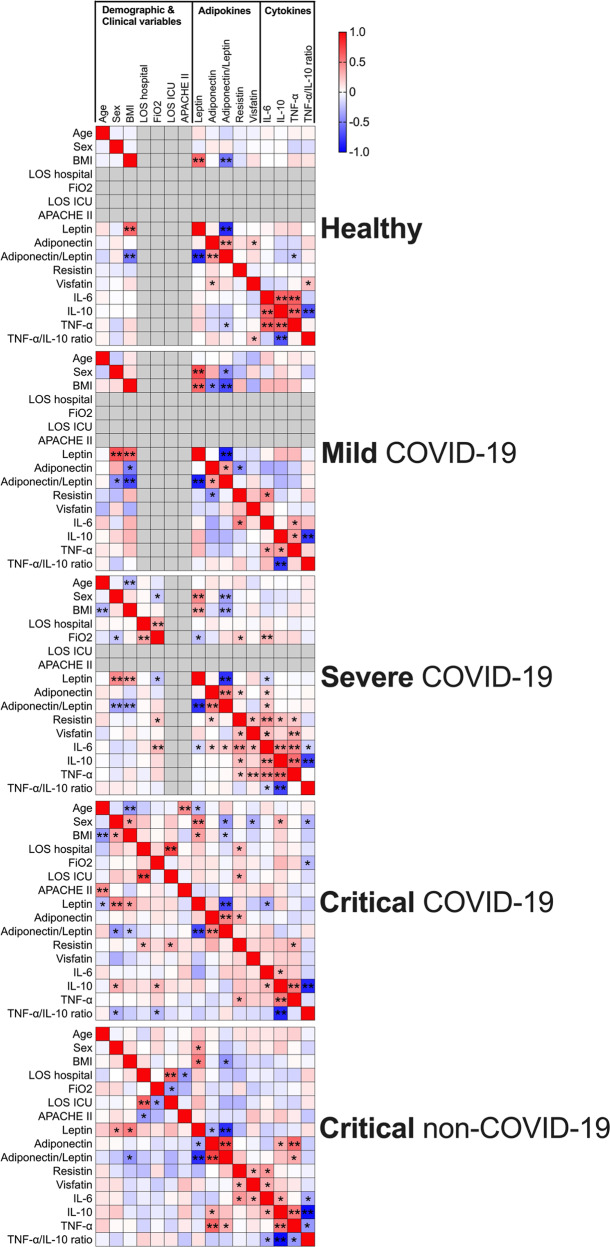
In this multi-centre prospective cross-sectional study, we collected blood samples and clinical data from COVID-19 patients. The severity of COVID-19 was classified as mild (no hospital admission), severe (ward admission), and critical (ICU admission). ICU non-COVID-19 patients were also included and plasma from healthy age, sex, and BMI-matched individuals obtained from Lifelines. Multi-analyte profiling of plasma adipokines (Leptin, Adiponectin, Resistin, Visfatin) and inflammatory markers (IL-6, TNFα, IL-10) were determined using Luminex multiplex assays.
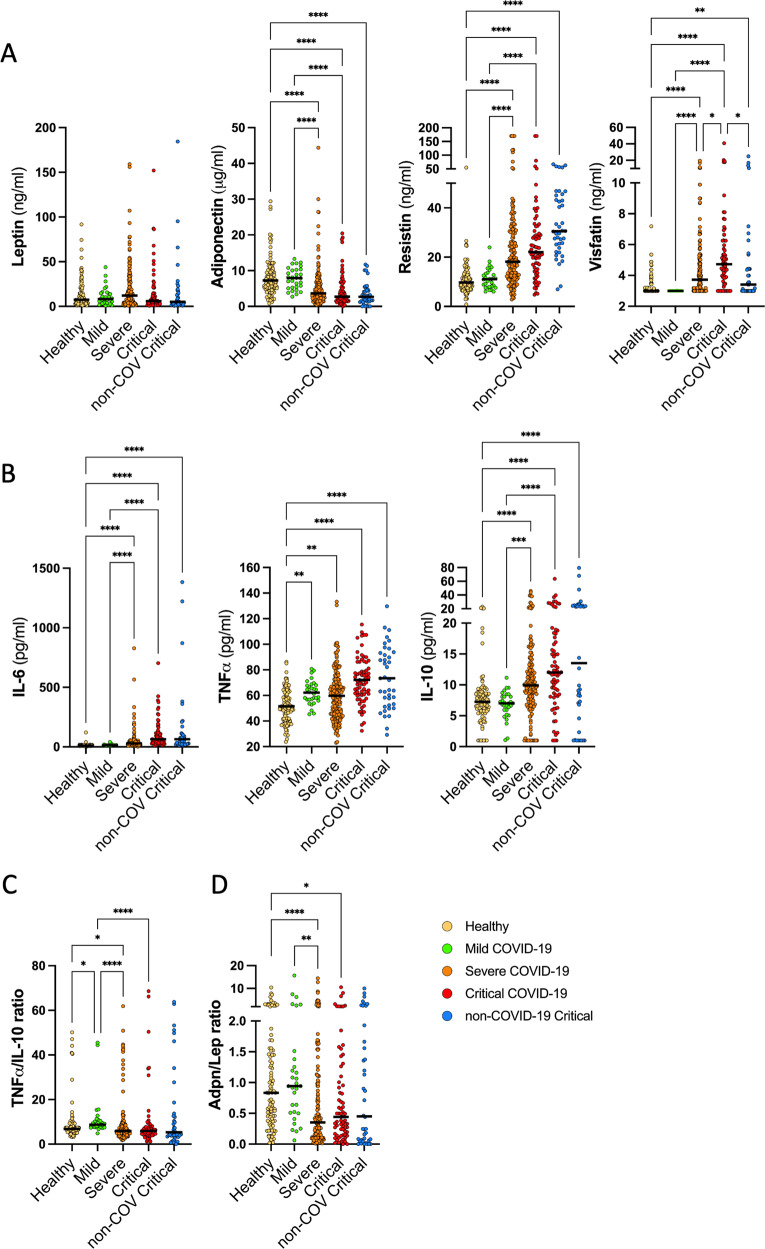
Between March and December 2020, 260 SARS-CoV-2 infected individuals (age: 65 [56-74] BMI 27.0 [24.4-30.6]) were included: 30 mild, 159 severe, and 71 critical patients. Circulating leptin levels were reduced in critically ill patients with a high BMI yet this decrease was absent in patients that were administered dexamethasone. Visfatin levels were higher in critical COVID-19 patients compared to non-COVID-ICU, mild and severe patients (4.7 vs 3.4, 3.0, and 3.72 ng/mL respectively, p < 0.05). Lower Adiponectin levels, but higher Resistin levels were found in severe and critical patients, compared to those that did not require hospitalization (3.65, 2.7 vs 7.9 µg/mL, p < 0.001, and 18.2, 22.0 vs 11.0 ng/mL p < 0.001).
Circulating adipokine levels are associated with COVID-19 hospitalization, i.e., the need for oxygen support (general ward), or the need for mechanical ventilation and other organ support in the ICU, but not mortality.
肥胖是 COVID-19 不良结局的一个危险因素,可能是由于脂肪因子和细胞因子的失调分泌导致慢性炎症状态所致。我们研究了血浆脂肪因子与 COVID-19 严重程度、全身炎症、临床参数和 COVID-19 患者预后之间的关系。
在这项多中心前瞻性横断面研究中,我们收集了 COVID-19 患者的血液样本和临床数据。COVID-19 的严重程度分为轻度(无需住院)、重度(病房住院)和危重症(ICU 住院)。还纳入了 ICU 中非 COVID-19 患者,并从 Lifelines 中获得了年龄、性别和 BMI 匹配的健康个体的血浆。使用 Luminex 多重分析测定血浆脂肪因子(瘦素、脂联素、抵抗素、内脂素)和炎症标志物(IL-6、TNFα、IL-10)的多分析物谱。
2020 年 3 月至 12 月期间,共纳入 260 例 SARS-CoV-2 感染患者(年龄:65 [56-74] BMI 27.0 [24.4-30.6]):30 例轻度、159 例重度和 71 例危重症患者。危重症高 BMI 患者的循环瘦素水平降低,但接受地塞米松治疗的患者则无此降低。与非 COVID-ICU、轻度和重度患者相比,危重症 COVID-19 患者的内脂素水平更高(4.7 与 3.4、3.0 和 3.72ng/mL,p<0.05)。与无需住院治疗的患者相比,重症和危重症患者的脂联素水平较低,抵抗素水平较高(3.65、2.7 与 7.9μg/mL,p<0.001,和 18.2、22.0 与 11.0ng/mL,p<0.001)。
循环脂肪因子水平与 COVID-19 住院相关,即需要氧支持(普通病房)或需要机械通气和 ICU 中的其他器官支持,但与死亡率无关。