Division of Vascular Surgery, University of Pittsburgh Medical Center, Pittsburgh, PA.
Division of Vascular Surgery, University of Pittsburgh Medical Center, Pittsburgh, PA.
J Vasc Surg. 2023 Apr;77(4):1165-1173.e1. doi: 10.1016/j.jvs.2022.12.002. Epub 2022 Dec 13.
Hypercoagulability is common in severe acute respiratory syndrome coronavirus 2 and has been associated with arterial thrombosis leading to acute limb ischemia (ALI). Our objective was to determine the outcomes of concurrent coronavirus disease 2019 (COVID-19) infection and ALI, particularly during the Delta variant surge and the impact of vaccination status.
A retrospective review was performed of patients treated at a single health care system between March 2020 and December 2021 for ALI and recent (<14 days) COVID-19 infection or who developed ALI during hospitalization for the same disease. Patients were grouped by year as well as by pre and post Delta variant emergence in 2021 based on the World Health Organization timeline (January to May vs June to December). Baseline demographics, imaging, interventions, and outcomes were evaluated. A control cohort of all patients with ALI requiring surgical intervention for a 2-year period prior to the pandemic was used for comparison. Primary outcomes were in-hospital mortality and amputation-free survival. Kaplan-Meier survival and Cox proportional hazards analysis were performed.
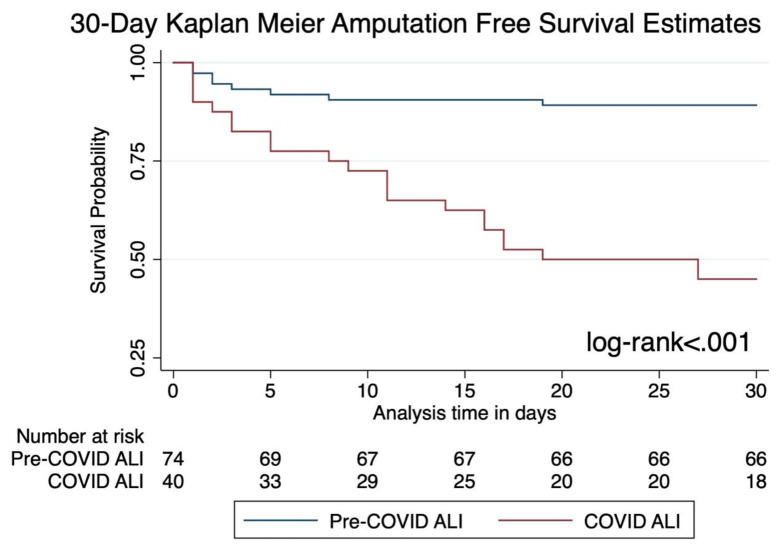
Forty acutely ischemic limbs were identified in 36 patients with COVID-19, the majority during the Delta surge (52.8%) and after the wide availability of vaccines. The rate of COVID-19-associated ALI, although low overall, nearly doubled during the Delta surge (0.37% vs 0.20%; P = .09). Intervention (open or endovascular revascularization vs primary amputation) was performed on 31 limbs in 28 individuals, with the remaining eight treated with systemic anti-coagulation. Postoperative mortality was 48%, and overall mortality was 50%. Major amputation following revascularization was significantly higher with COVID-19 ALI (25% vs 3%; P = .006) compared with the pre-pandemic group. Thirty-day amputation-free survival was significantly lower (log-rank P < .001). COVID-19 infection (adjusted hazard ratio, 6.2; P < .001) and age (hazard ratio, 1.1; P = .006) were associated with 30-day amputation in multivariate analysis. Severity of COVID-19 infection, defined as vasopressor usage, was not associated with post-revascularization amputation. There was a higher incidence of re-thrombosis in the latter half of 2021 with the Delta surge, as reintervention for recurrent ischemia of the same limb was more common than our previous experience (21% vs 0%; P = .55). COVID-19-associated limb ischemia occurred almost exclusively in non-vaccinated patients (92%).
ALI observed with Delta appears more resistant to standard therapy. Unvaccinated status correlated highly with ALI occurrence in the setting of COVID-19 infection. Information of limb loss as a COVID-19 complication among non-vaccinated patients may help to increase compliance.
严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2)中存在高凝状态,并与导致急性肢体缺血(ALI)的动脉血栓形成有关。我们的目的是确定同时患有 COVID-19 (新冠肺炎)和 ALI 的患者的结局,特别是在 Delta 变异株流行期间,以及疫苗接种状况的影响。
对 2020 年 3 月至 2021 年 12 月期间在单一医疗系统接受治疗的 ALI 患者进行了回顾性研究,这些患者的 ALI 是由近期(<14 天)的 COVID-19 感染或在同一疾病住院期间发生的 ALI 引起的。根据世界卫生组织的时间线(2021 年 1 月至 5 月与 6 月至 12 月),患者按年份以及在 2021 年 Delta 变异株出现前后(分为前 Delta 期和后 Delta 期)分组。评估了患者的基线人口统计学、影像学、干预措施和结局。还使用了所有在大流行前 2 年期间因 ALI 需要手术干预的患者作为对照队列进行比较。主要结局是住院期间死亡率和免于截肢的生存率。进行 Kaplan-Meier 生存分析和 Cox 比例风险分析。
在 36 名 COVID-19 患者中,共发现 40 条急性缺血肢体,其中大多数发生在 Delta 变异株流行期间(52.8%)和疫苗广泛使用之后。虽然总体上 COVID-19 相关的 ALI 发生率较低,但在 Delta 变异株流行期间几乎翻了一番(0.37% vs 0.20%;P=.09)。28 名患者中的 31 条肢体接受了干预(开放或血管内血运重建术与初次截肢),其余 8 名患者接受了全身抗凝治疗。术后死亡率为 48%,总死亡率为 50%。与大流行前组相比,COVID-19 相关的 ALI 接受血运重建后的主要截肢率明显更高(25% vs 3%;P=.006)。30 天免于截肢的生存率明显较低(对数秩检验 P<.001)。COVID-19 感染(调整后的风险比,6.2;P<.001)和年龄(风险比,1.1;P=.006)是多变量分析中 30 天内截肢的相关因素。COVID-19 感染的严重程度(定义为血管加压药的使用)与血运重建后的截肢无关。随着 Delta 变异株的出现,2021 年下半年的再血栓形成发生率更高,同一肢体的复发性缺血需要再次干预的情况比我们之前的经验更常见(21% vs 0%;P=.55)。与 COVID-19 相关的肢体缺血几乎仅发生在未接种疫苗的患者(92%)中。
在 Delta 变异株流行期间观察到的 ALI 似乎对标准治疗更具抵抗力。未接种疫苗的状态与 COVID-19 感染中 ALI 的发生高度相关。非接种疫苗患者的肢体丧失作为 COVID-19 并发症的信息可能有助于提高接种率。