Department of Internal Medicine, University Hospitals Cleveland Medical Center, Cleveland, OH, USA.
Mainz University Medical Center, Mainz, Rhineland-Palatinate, Germany.
J Thromb Thrombolysis. 2023 Feb;55(2):228-242. doi: 10.1007/s11239-022-02750-1. Epub 2022 Dec 19.
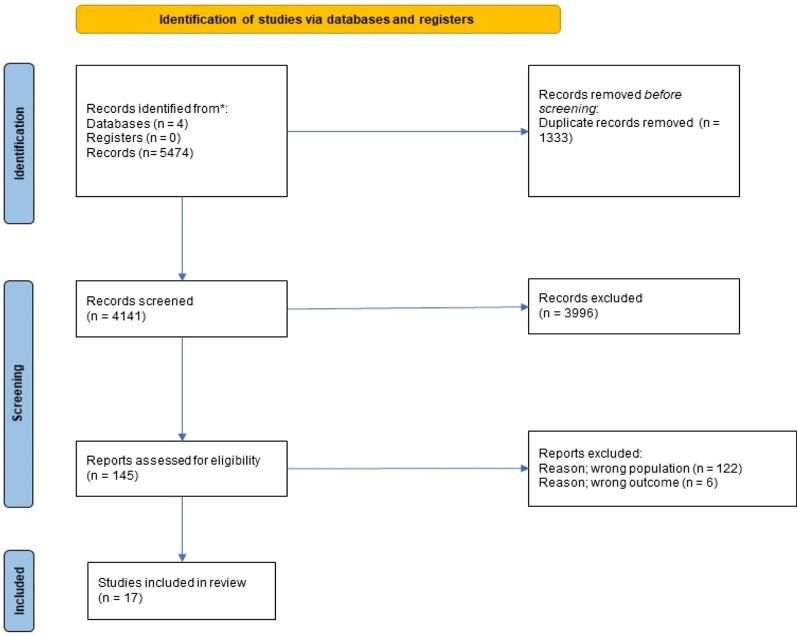
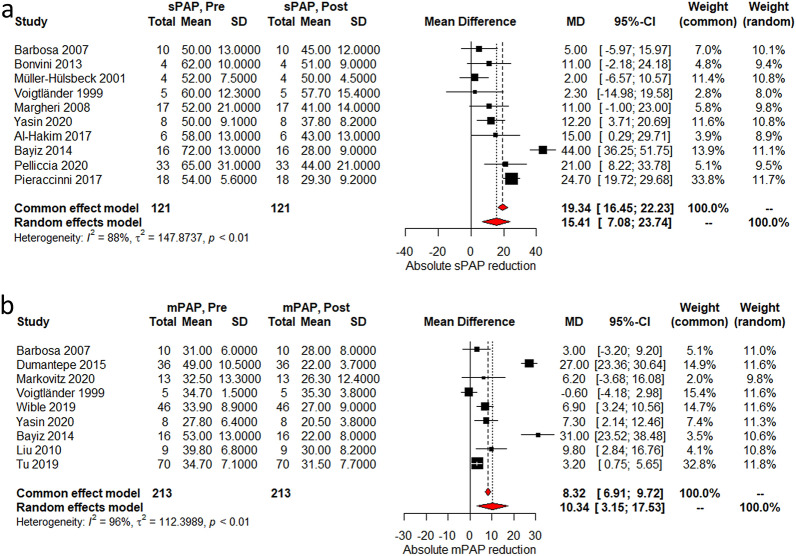
Catheter-directed interventions have slowly been gaining ground in the treatment of pulmonary embolism (PE), especially in patients with increased risk of bleeding. The goal of this study is to summarize the evidence for the efficacy and safety of percutaneous thrombectomy (PT) in patients with contraindications to systemic and local thrombolysis. We performed a systematic review and meta-analysis using MEDLINE, Cochrane, Scopus and the Web of Science databases for studies from inception to March 2022. We included patients with intermediate- and high-risk PE with contraindications to thrombolysis; patients who received systematic or local thrombolysis were excluded. Primary endpoint was in-hospital and 30-day mortality, with secondary outcomes based on hemodynamic and radiographic changes. Major bleeding events were assessed as a safety endpoint. Seventeen studies enrolled 455 patients, with a mean age of 58.6 years and encompassing 50.4% females. In-hospital and 30-day mortality rates were 4% (95% CI 3-6%) and 5% (95% CI 3-9%) for all-comers, respectively. We found a post-procedural reduction in systolic and mean pulmonary arterial pressures by 15.4 mmHg (95% CI 7-23.7) and 10.3 mmHg (95% CI 3.1-17.5) respectively. The RV/LV ratio and Miller Index were reduced by 0.42 (95% CI 0.38-46) and 7.8 (95% CI 5.2-10.5). Major bleeding events occurred in 4% (95% CI 3-6%). This is the first meta-analysis to report pooled outcomes on PT in intermediate- and high-risk PE patients without the use of systemic or local thrombolytics. The overall mortality rate is comparable to other contemporary treatments, and is an important modality particularly in those with contraindications for adjunctive thrombolytic therapy. Further studies are needed to understand the interplay of anticoagulation with PT and catheter-directed thrombolysis.
经导管介入治疗在肺栓塞(PE)的治疗中逐渐得到认可,尤其是在有出血风险增加的患者中。本研究旨在总结经皮血栓切除术(PT)在溶栓禁忌的中高危 PE 患者中的疗效和安全性证据。我们使用 MEDLINE、Cochrane、Scopus 和 Web of Science 数据库进行了系统评价和荟萃分析,检索时间从建库至 2022 年 3 月。我们纳入了有溶栓禁忌的中高危 PE 患者;排除接受系统性或局部溶栓治疗的患者。主要终点是住院和 30 天死亡率,次要终点基于血流动力学和影像学变化。主要出血事件作为安全性终点进行评估。17 项研究共纳入 455 例患者,平均年龄 58.6 岁,女性占 50.4%。所有患者的住院和 30 天死亡率分别为 4%(95%CI 3-6%)和 5%(95%CI 3-9%)。我们发现,术后收缩压和平均肺动脉压分别降低 15.4mmHg(95%CI 7-23.7)和 10.3mmHg(95%CI 3.1-17.5)。右心室/左心室比值和 Miller 指数分别降低 0.42(95%CI 0.38-46)和 7.8(95%CI 5.2-10.5)。主要出血事件发生率为 4%(95%CI 3-6%)。这是第一项报告在不使用全身或局部溶栓的情况下,对中高危 PE 患者进行 PT 汇总结局的荟萃分析。总的死亡率与其他当代治疗方法相当,在有辅助溶栓治疗禁忌的患者中是一种重要的治疗方式。需要进一步研究以了解抗凝与 PT 和导管内溶栓的相互作用。