Department of Cardiology Rinku General Medical Center Osaka Japan.
Division of Cardiology Osaka General Medical Center Osaka Japan.
J Am Heart Assoc. 2023 Jan 3;12(1):e026326. doi: 10.1161/JAHA.122.026326. Epub 2022 Dec 24.
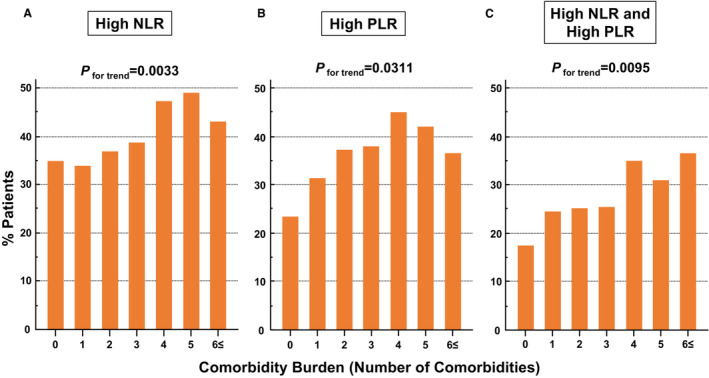
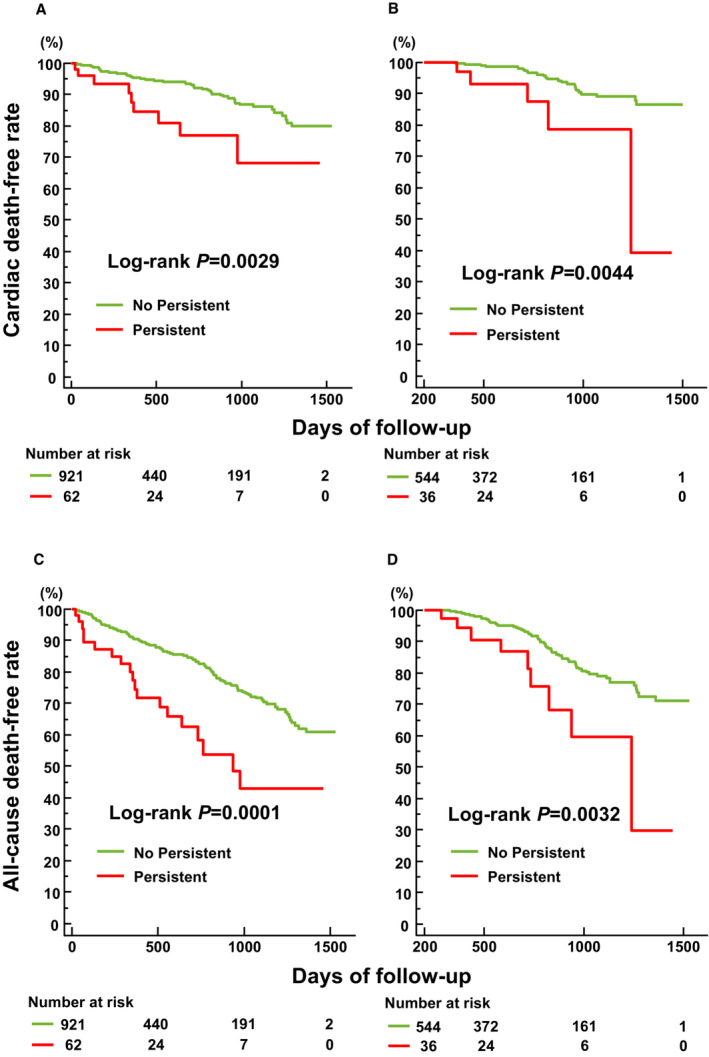
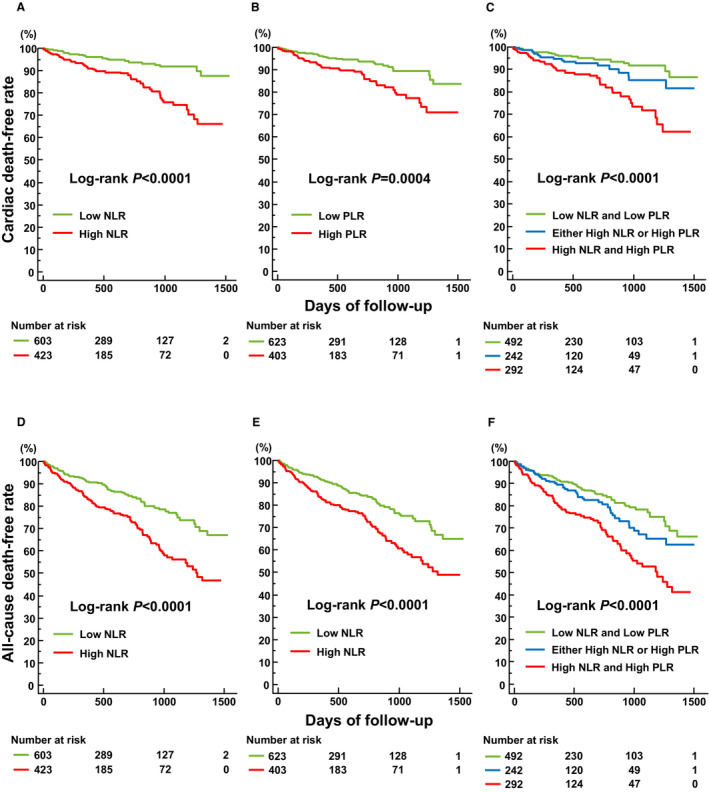
Background Neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) are novel inflammation markers. Their combined usefulness for estimating the prognosis of patients with heart failure with preserved ejection fraction (HFpEF) admitted for acute decompensated heart failure remains elusive. Methods and Results We investigated 1026 patients registered in the Prospective Multicenter Observational Study of Patients with Heart Failure with Preserved Ejection Fraction. Both NLR and PLR values were measured at the time of admission. Comorbidity burden was defined as the number of occurrences of 8 common comorbidities of HFpEF. The primary end point was cardiac death. The patients were stratified into 3 groups based on the optimal cut-off values of NLR and PLR on the receiver operating characteristic curve analysis for predicting cardiac death (low NLR and PLR, either high NLR or PLR, and both high NLR and PLR). After a median follow-up of 429 days, 195 patients died, with 85 of these deaths attributed to cardiac causes. An increased comorbidity burden was significantly associated with a higher proportion of patients with high NLR (>4.5) or PLR (>193), or both. High NLR and PLR values were independently associated with cardiac death, and a combination of both values was the strongest predictor (hazard ratio, 2.66 [95% CI, 1.51%-4.70%], =0.0008). A significant difference was found in the rate of cardiac death among the 3 groups stratified by NLR and PLR values. Conclusions The combination of NLR and PLR is useful for the prediction of postdischarge cardiac death in patients with acute HFpEF. Registration URL: ClinicalTrials.gov; Unique identifier: UMIN000021831.
中性粒细胞与淋巴细胞比值(NLR)和血小板与淋巴细胞比值(PLR)是新型炎症标志物。它们联合用于评估因急性失代偿性心力衰竭而住院的射血分数保留的心力衰竭(HFpEF)患者的预后,其作用仍不清楚。
我们调查了在前瞻性多中心观察性研究中注册的 1026 例 HFpEF 患者。入院时测量 NLR 和 PLR 值。共病负担定义为 HFpEF 的 8 种常见共病发生次数。根据 NLR 和 PLR 的最佳截断值对患者进行分层,以预测心脏死亡(低 NLR 和 PLR、高 NLR 或 PLR 或两者均高)。中位随访 429 天后,195 例患者死亡,其中 85 例死于心脏原因。共病负担增加与更高比例的患者出现高 NLR(>4.5)或 PLR(>193)或两者均高显著相关。高 NLR 和 PLR 值与心脏死亡独立相关,两者结合是最强的预测因素(危险比,2.66[95%置信区间,1.51%-4.70%],=0.0008)。根据 NLR 和 PLR 值分层的 3 组之间,心脏死亡发生率存在显著差异。
NLR 和 PLR 的联合应用有助于预测急性 HFpEF 患者出院后的心脏死亡。
ClinicalTrials.gov;唯一标识符:UMIN000021831。