Hrubaru Ingrid, Motoc Andrei, Bratosin Felix, Rosca Ovidiu, Folescu Roxana, Moise Marius Liviu, Neagoe Octavian, Citu Ioana Mihaela, Feciche Bogdan, Gorun Florin, Erdelean Dragos, Ratiu Adrian, Citu Cosmin
Department of Obstetrics and Gynecology, "Victor Babes" University of Medicine and Pharmacy Timisoara, Eftimie Murgu Square 2, 300041 Timisoara, Romania.
Doctoral School, "Victor Babes" University of Medicine and Pharmacy Timisoara, Eftimie Murgu Square 2, 300041 Timisoara, Romania.
J Pers Med. 2022 Nov 8;12(11):1871. doi: 10.3390/jpm12111871.
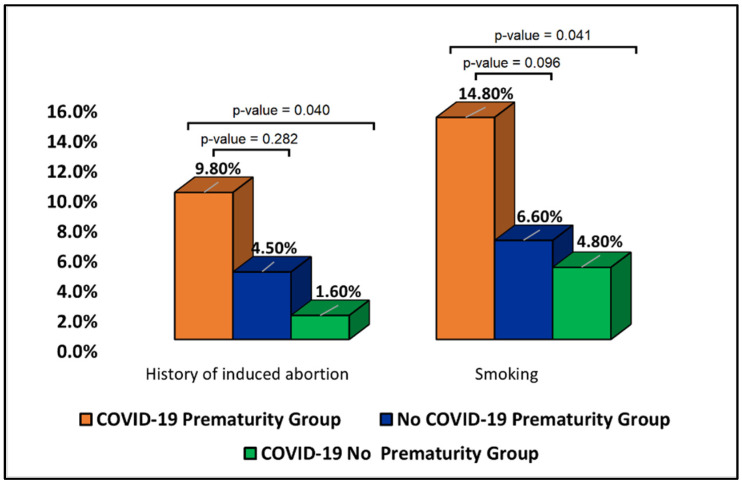
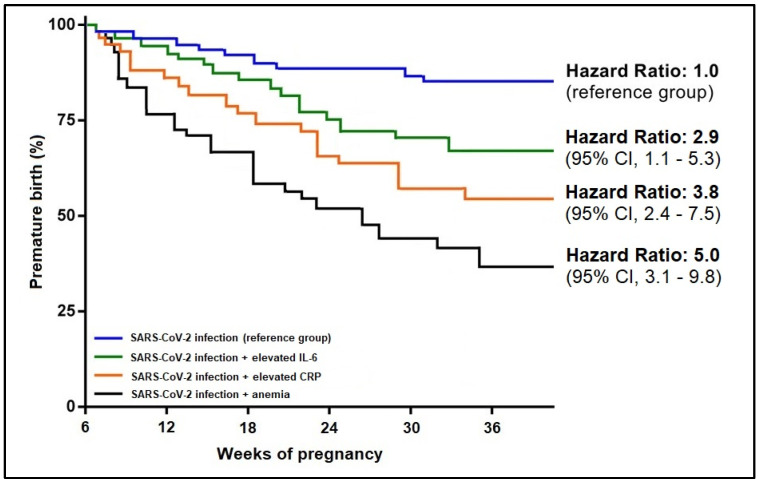
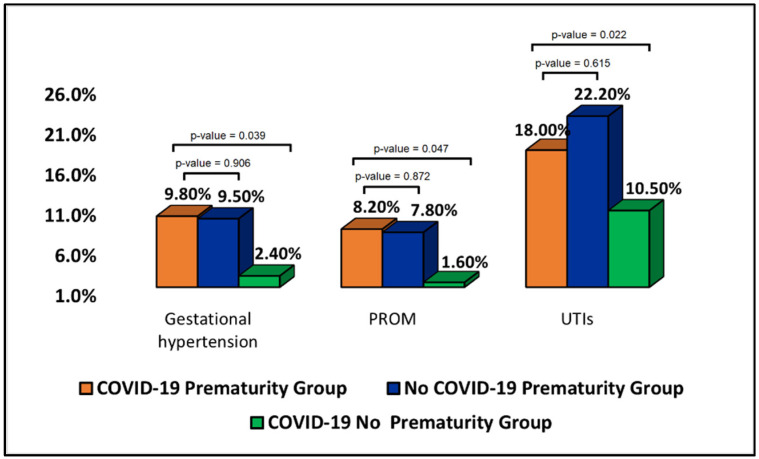
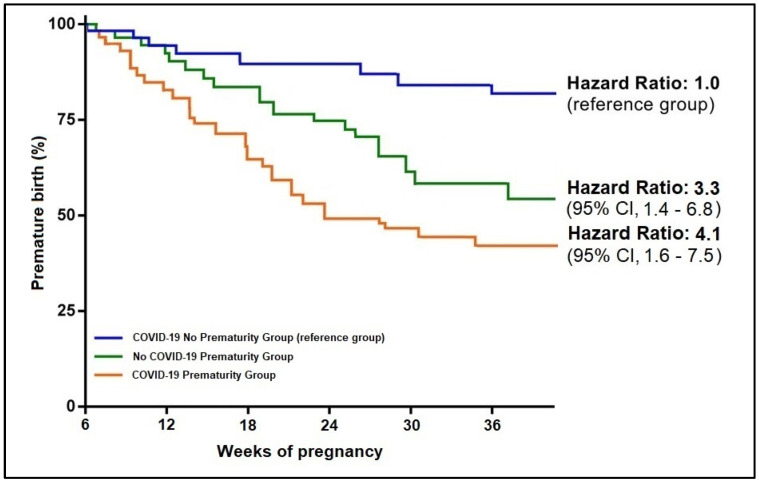
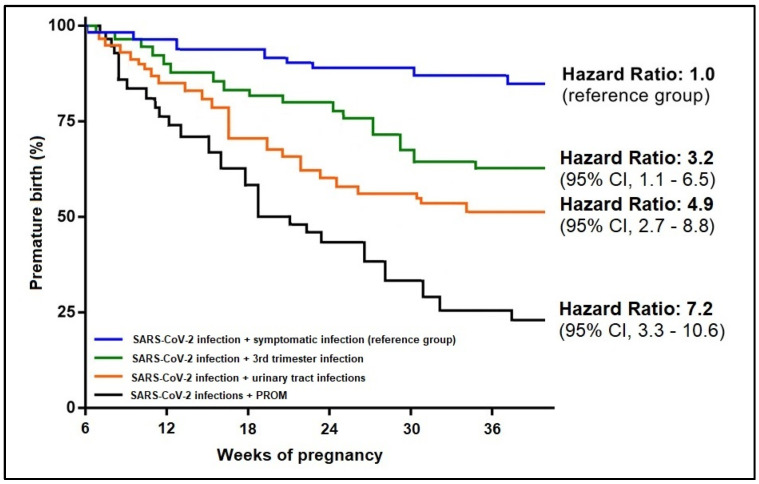
Studies observed that women infected with SARS-CoV-2 during pregnancy had a higher risk of preterm birth. Although it is likely that COVID-19 during the late trimester of pregnancy can trigger premature birth, prematurity remains a concern, and it is vital to study additional clinical and biological patient factors that are highly associated with this negative pregnancy outcome and allow for better management based on the existing predictors. In order to achieve this goal, the current study retrospectively recruited 428 pregnant patients that were separated into three study groups using a 1:2:4 matching ratio and a nearest-neighbor matching method. Sixty-one pregnant patients had a history of COVID-19 during pregnancy and gave birth prematurely; 124 pregnant patient controls had COVID-19 and gave birth full-term, while the second control group of 243 pregnant patients had a premature birth but no history of COVID-19. It was observed that a symptomatic SARS-CoV-2 infection during the third trimester was significantly more likely to be associated with premature birth. Even though the rate of ICU admission was higher in these cases, the mortality rate did not change significantly in the COVID-19 groups. However, SARS-CoV-2 infection alone did not show statistical significance in determining a premature birth (β = 1.09, CI = 0.94−1.15, p-value = 0.067). Maternal anemia was the strongest predictor for prematurity in association with SARS-CoV-2 infection (β = 3.65, CI = 1.46−5.39, p-value < 0.001), followed by elevated CRP (β = 2.11, CI = 1.20−3.06, p-value < 0.001), and respectively IL-6 (β = 1.92, CI = 1.20−2.47, p-value = 0.001. SARS-CoV-2 infection is associated with an increased risk of preterm birth, as shown by our data. If SARS-CoV-2 infection arises during the third trimester, it is recommended that these patients be hospitalized for surveillance of clinical evolution and biological parameters, such as anemia and high inflammatory markers, which have a multiplicative influence on the pregnancy result.
研究观察到,孕期感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的女性早产风险更高。虽然妊娠晚期的2019冠状病毒病(COVID-19)很可能会引发早产,但早产仍是一个令人担忧的问题,研究与这种不良妊娠结局高度相关的其他临床和生物学患者因素,并基于现有预测指标进行更好的管理至关重要。为了实现这一目标,本研究回顾性招募了428名孕妇,采用1:2:4的匹配比例和最近邻匹配法将其分为三个研究组。61名孕妇在孕期有COVID-19病史且早产;124名孕妇对照组有COVID-19且足月分娩,而243名孕妇的第二对照组早产但无COVID-19病史。据观察,妊娠晚期有症状的SARS-CoV-2感染更有可能与早产相关。尽管这些病例的重症监护病房(ICU)入院率较高,但COVID-19组的死亡率没有显著变化。然而,仅SARS-CoV-2感染在确定早产方面未显示出统计学意义(β=1.09,可信区间[CI]=0.94−1.15,P值=0.067)。与SARS-CoV-2感染相关的早产最强预测因素是母体贫血(β=3.65,CI=1.46−5.39,P值<0.001),其次是C反应蛋白(CRP)升高(β=2.11,CI=1.20−3.06,P值<0.001),以及白细胞介素-6(IL-6)(β=1.92,CI=1.20−2.47,P值=0.001)。我们的数据表明,SARS-CoV-2感染与早产风险增加相关。如果在妊娠晚期出现SARS-CoV-2感染,建议将这些患者住院,监测临床进展和生物学参数,如贫血和高炎症标志物,这些因素会对妊娠结局产生倍增影响。