Northwestern University-The Feinberg School of Medicine, Chicago, Illinois, USA.
Arbor Research Collaborative for Health, Ann Arbor, Michigan, USA.
Neurourol Urodyn. 2023 Jan;42(1):194-204. doi: 10.1002/nau.25067. Epub 2022 Oct 23.
Limited epidemiological data exist describing how patients engage with various treatments for overactive bladder (OAB). To improve care for patients with OAB, it is essential to gain a better understanding of how patients interface with OAB treatments longitudinally, that is, how often patients change treatments and the pattern of this treatment change in terms of escalation and de-escalation.
To describe treatment patterns for women with bothersome urinary urgency (UU) and/or urgency urinary incontinence (UUI) presenting to specialty care over 1 year.
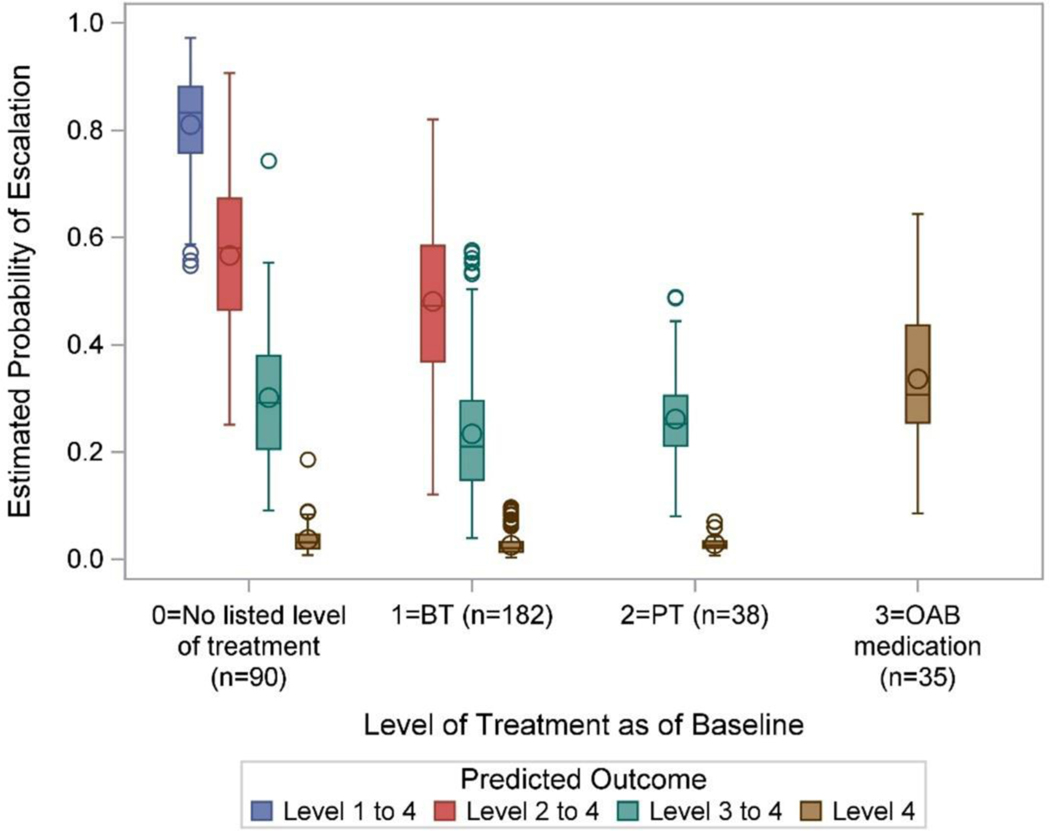
The Symptoms of Lower Urinary Tract Dysfunction Research Network (LURN) study enrolled adult women with bothersome UU and/or UUI seeking care for lower urinary tract symptoms (LUTS) between January 2015 and September 2016. An ordinal logistic regression model was fitted to describe the probabilities of escalating or de-escalating level of treatment during 1-year follow-up.
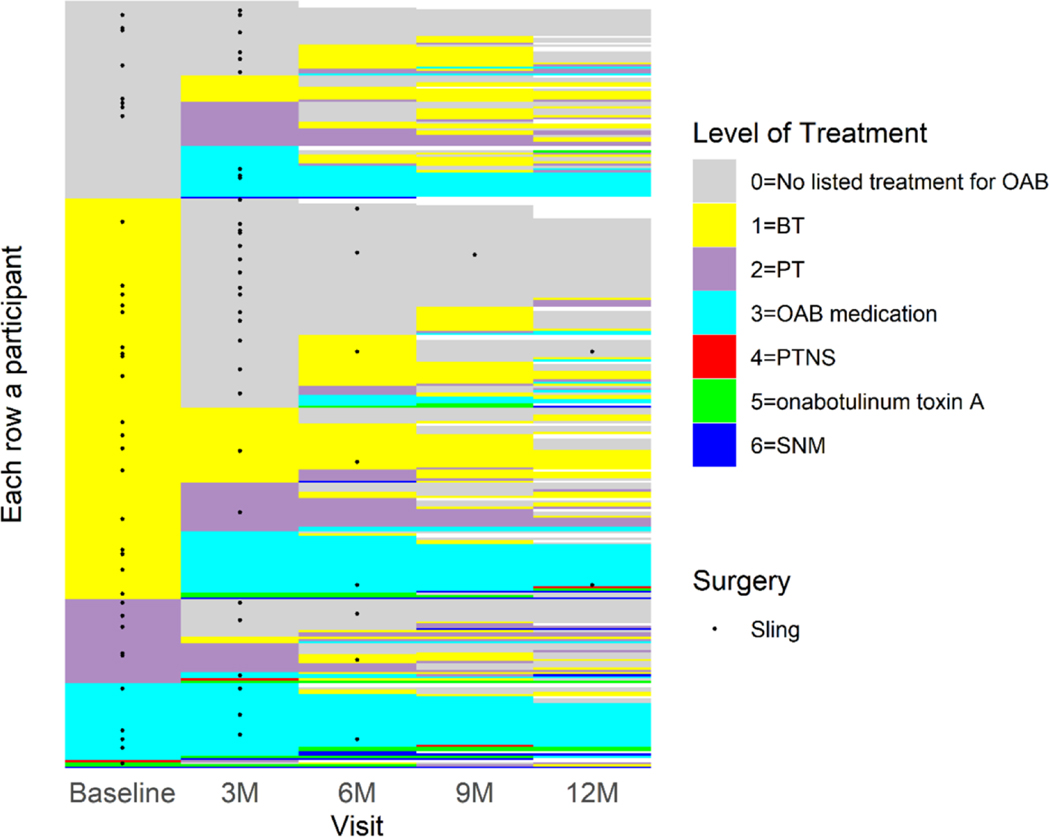
Among 349 women, 281 reported UUI and 68 reported UU at baseline. At the end of 1 year of treatment by a urologist or urogynecologist, the highest level of treatment received by participants was 5% expectant management, 36% behavioral treatments (BT), 26% physical therapy (PT), 26% OAB medications, 1% percutaneous tibial nerve stimulation, 3% intradetrusor onabotulinum toxin A injection, and 3% sacral neuromodulation. Participants using BT or PT at baseline were more likely to be de-escalated to no treatment than participants on OAB medications at baseline, who tended to stay on medications. Predictors of the highest level of treatment included starting level of treatment, hypertension, UUI severity, stress urinary incontinence, and anticholinergic burden score.
Treatment patterns for UU and UUI are diverse. Even for patients with significant bother from OAB presenting to specialty clinics, further treatment often only involves conservative or medical therapies. This study highlights the need for improved treatment algorithms to escalate patients with persistent symptoms, or to adjust care in those who have been unsuccessfully treated.
目前仅有有限的流行病学数据描述了患者如何接受各种治疗方案来治疗膀胱过度活动症(OAB)。为了改善 OAB 患者的护理,必须更好地了解患者如何从纵向角度与 OAB 治疗方案进行交互,即患者多久更换一次治疗方案,以及在升级和降级方面的治疗方案变化模式。
描述在 1 年内因烦扰性尿急(UU)和/或急迫性尿失禁(UUI)就诊于专科门诊的女性患者的治疗模式。
下尿路功能障碍症状研究网络(LURN)研究纳入了 2015 年 1 月至 2016 年 9 月期间因下尿路症状(LUTS)寻求治疗的烦扰性 UU 和/或 UUI 的成年女性。采用有序逻辑回归模型来描述在 1 年随访期间升级或降级治疗水平的概率。
在 349 名女性中,281 名报告了基线时有 UUI,68 名报告了 UU。在接受泌尿科医生或泌尿妇科医生治疗 1 年后,参与者接受的最高治疗水平为 5%的期待管理、36%的行为治疗(BT)、26%的物理治疗(PT)、26%的 OAB 药物治疗、1%的经皮胫神经刺激、3%的膀胱内注射肉毒杆菌毒素 A、3%的骶神经调节。与基线时使用 OAB 药物治疗的参与者相比,基线时使用 BT 或 PT 的参与者更有可能降级为无治疗,而基线时使用 OAB 药物治疗的参与者更有可能继续使用药物。最高治疗水平的预测因素包括起始治疗水平、高血压、UUI 严重程度、压力性尿失禁和抗胆碱能药物负担评分。
UU 和 UUI 的治疗模式多种多样。即使是因 OAB 而出现严重困扰就诊于专科诊所的患者,进一步的治疗通常也只涉及保守或药物治疗。本研究强调了需要改进治疗方案,以对持续性症状的患者进行升级治疗,或对治疗效果不佳的患者调整治疗方案。