Department of Pharmacy, University of Washington School of Pharmacy, Seattle.
Division of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of California, San Diego, La Jolla.
JAMA Netw Open. 2023 Jan 3;6(1):e2249370. doi: 10.1001/jamanetworkopen.2022.49370.
Prevalent use of antihypertensive medications that stimulate type 2 and 4 angiotensin II receptors, compared with those that do not stimulate these receptors, has been associated with a lower risk of dementia. However, previous studies were limited by inclusion of individuals with prevalent hypertension and a history of antihypertensive use prior to the start of the study, which can introduce bias.
To examine the association of new use of antihypertensive medication regimens that stimulate vs inhibit type 2 and 4 angiotensin II receptors with Alzheimer disease and related dementias (ADRD) among Medicare beneficiaries.
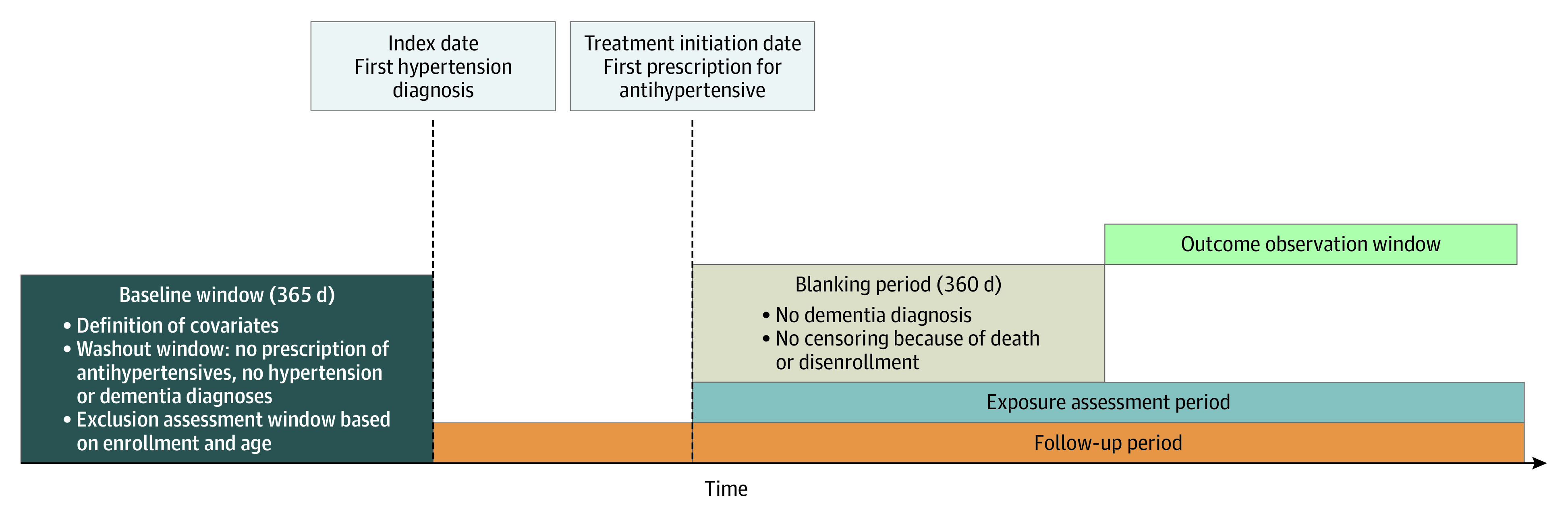
DESIGN, SETTING, AND PARTICIPANTS: This cohort study was conducted among 57 773 Medicare fee-for-service beneficiaries (January 1, 2006, through December 31, 2018) aged 65 years or older with incident hypertension. Data analysis was conducted from January 1 through June 30, 2022.
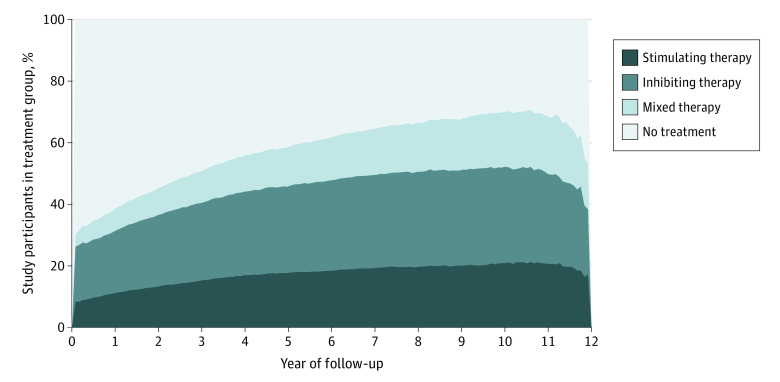
Initiation of antihypertensive medication regimens that stimulate or inhibit type 2 and 4 angiotensin II receptors, or mixed regimens (both stimulating and inhibiting), with the time-dependent measure being each 30-day interval.
The primary outcome was time to first occurrence of ADRD (Centers for Medicare & Medicaid Services Chronic Conditions Data Warehouse definition). Cox proportional hazards regression modeling with time-dependent variables was performed to estimate the association between time-dependent treatment groups and time to ADRD, after adjusting for sociodemographic and clinical characteristics.
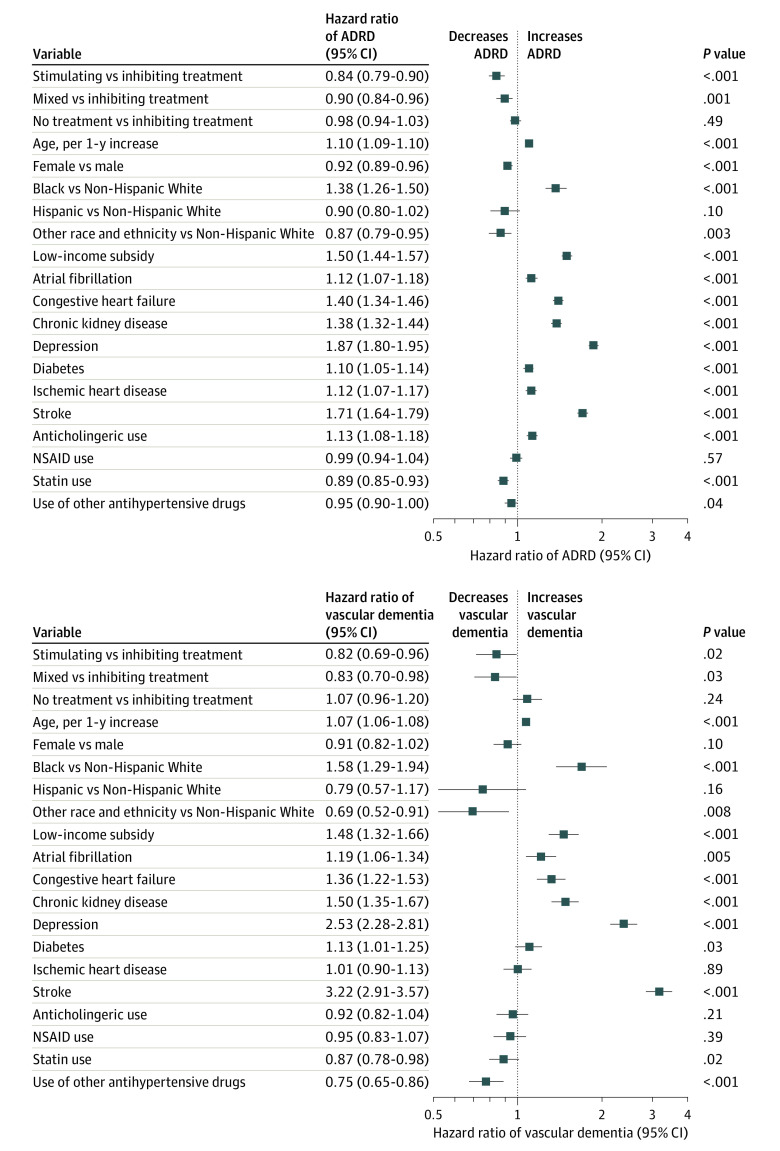
The sample included 57 773 Medicare beneficiaries (36 348 women [62.9%]; mean [SD] age, 73.8 [6.3] years; 2954 [5.1%] Black, 1545 [2.7%] Hispanic; 50 184 [86.9%] White, and 3090 [5.4%] Other individuals [the Other category included individuals of American Indian, Asian, other, or unknown race and ethnicity]). During a median of 6.9 years (IQR, 4.7-9.3 years) of follow-up, the unadjusted incidence density rate of ADRD was 2.2 cases per 100 person-years (95% CI, 2.1-2.4 cases per 100 person-years) for the group receiving regimens that stimulate type 2 and 4 angiotensin II receptors compared with 3.1 cases per 100 person-years (95% CI, 3.0-3.2 cases per 100 person-years) for the group receiving regimens that inhibit type 2 and 4 angiotensin II receptors and 2.7 cases per 100 person-years (95% CI, 2.6-2.9 cases per 100 person-years) for the group receiving mixed treatment regimens. In adjusted Cox proportional hazards regression modeling, stimulating treatment was associated with a statistically significant 16% reduction in the hazard of ADRD compared with inhibiting treatment (hazard ratio, 0.84; 95% CI, 0.79-0.90). Mixed regimen use was also associated with reduced hazards of ADRD compared with the inhibiting group (hazard ratio, 0.90; 95% CI, 0.84-0.96).
This cohort study of Medicare beneficiaries suggests that use of antihypertensive medications that stimulate type 2 and 4 angiotensin II receptors was associated with lower risk of ADRD compared with antihypertensive medications that inhibit these receptors. Confirmation is needed in a randomized trial.
与不刺激这些受体的降压药物相比,使用刺激 2 型和 4 型血管紧张素 II 受体的降压药物与痴呆风险降低相关。然而,先前的研究受到纳入有既往高血压和在研究开始前使用过降压药物的个体的限制,这可能会引入偏倚。
在 Medicare 受益人中,检查新使用刺激 vs 抑制 2 型和 4 型血管紧张素 II 受体的降压药物与阿尔茨海默病和相关痴呆(ADRD)之间的关联。
设计、设置和参与者:这项队列研究纳入了 57773 名年龄在 65 岁或以上、有新发高血压的 Medicare 收费服务受益人(2006 年 1 月 1 日至 2018 年 12 月 31 日)。数据分析于 2022 年 1 月 1 日至 6 月 30 日进行。
使用刺激或抑制 2 型和 4 型血管紧张素 II 受体的降压药物方案,或混合方案(刺激和抑制),时间依赖性测量为每个 30 天间隔。
主要结局是首次发生 ADRD 的时间(Medicare & Medicaid Services 慢性病数据仓库定义)。使用时间依赖性变量的 Cox 比例风险回归模型,在调整社会人口统计学和临床特征后,估计时间依赖性治疗组与 ADRD 时间之间的关联。
该样本包括 57773 名 Medicare 受益人(36348 名女性[62.9%];平均[SD]年龄 73.8[6.3]岁;2954 名[5.1%]黑人,1545 名[2.7%]西班牙裔;50184 名[86.9%]白人,和 3090 名[5.4%]其他个体[其他类别包括美洲印第安人、亚洲人、其他或未知种族和民族的个体])。在中位 6.9 年(IQR,4.7-9.3 年)的随访期间,与抑制 2 型和 4 型血管紧张素 II 受体的药物相比,接受刺激 2 型和 4 型血管紧张素 II 受体药物的人群的 ADRD 发生率为每 100 人年 2.2 例(95%CI,每 100 人年 2.1-2.4 例),而接受抑制 2 型和 4 型血管紧张素 II 受体药物的人群的发生率为每 100 人年 3.1 例(95%CI,每 100 人年 3.0-3.2 例),接受混合治疗方案的人群的发生率为每 100 人年 2.7 例(95%CI,每 100 人年 2.6-2.9 例)。在调整后的 Cox 比例风险回归模型中,与抑制治疗相比,刺激治疗与 ADRD 风险降低统计学显著相关(风险比,0.84;95%CI,0.79-0.90)。与抑制组相比,混合方案的使用也与 ADRD 风险降低相关(风险比,0.90;95%CI,0.84-0.96)。
这项对 Medicare 受益人的队列研究表明,与抑制这些受体的降压药物相比,使用刺激 2 型和 4 型血管紧张素 II 受体的降压药物与 ADRD 风险降低相关。需要在随机试验中进行确认。