Department of Pharmacy, The Comparative Health Outcomes, Policy, and Economics (CHOICE) Institute, University of Washington, Seattle, WA, United States of America.
School of Pharmacy, Schaeffer Center for Health Policy and Economics, University of Southern California, Los Angeles, CA, United States of America.
PLoS One. 2020 Mar 4;15(3):e0229541. doi: 10.1371/journal.pone.0229541. eCollection 2020.
Hyperlipidemia and hypertension are modifiable risk factors for Alzheimer's disease and related dementias (ADRD). Approximately 25% of adults over age 65 use both antihypertensives (AHTs) and statins for these conditions. While a growing body of evidence found statins and AHTs are independently associated with lower ADRD risk, no evidence exists on simultaneous use for different drug class combinations and ADRD risk. Our primary objective was to compare ADRD risk associated with concurrent use of different combinations of statins and antihypertensives.
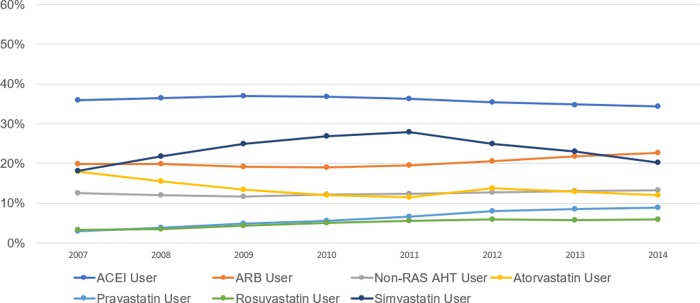
In a retrospective cohort study (2007-2014), we analyzed 694,672 Medicare beneficiaries in the United States (2,017,786 person-years) who concurrently used both statins and AHTs. Using logistic regression adjusting for age, socioeconomic status and comorbidities, we quantified incident ADRD diagnosis associated with concurrent use of different statin molecules (atorvastatin, pravastatin, rosuvastatin, and simvastatin) and AHT drug classes (two renin-angiotensin system (RAS)-acting AHTs, angiotensin converting enzyme inhibitors (ACEIs) or angiotensin-II receptor blockers (ARBs), vs non-RAS-acting AHTs).
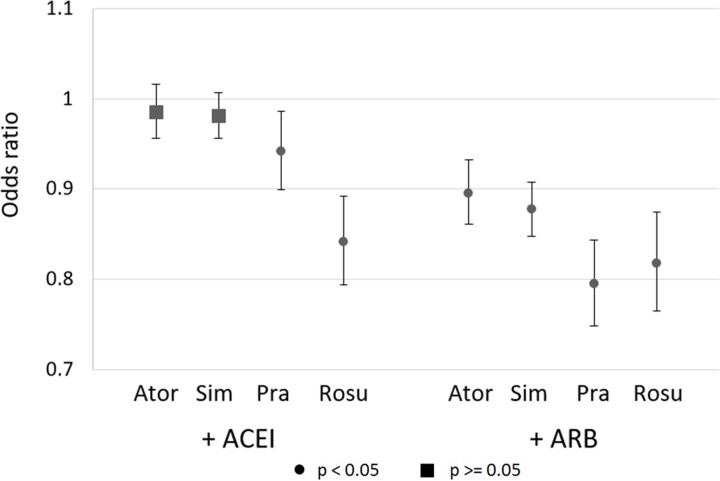
Pravastatin or rosuvastatin combined with RAS-acting AHTs reduce risk of ADRD relative to any statin combined with non-RAS-acting AHTs: ACEI+pravastatin odds ratio (OR) = 0.942 (CI: 0.899-0.986, p = 0.011), ACEI+rosuvastatin OR = 0.841 (CI: 0.794-0.892, p<0.001), ARB+pravastatin OR = 0.794 (CI: 0.748-0.843, p<0.001), ARB+rosuvastatin OR = 0.818 (CI: 0.765-0.874, p<0.001). ARBs combined with atorvastatin and simvastatin are associated with smaller reductions in risk, and ACEI with no risk reduction, compared to when combined with pravastatin or rosuvastatin. Among Hispanics, no combination of statins and RAS-acting AHTs reduces risk relative to combinations of statins and non-RAS-acting AHTs. Among blacks using ACEI+rosuvastatin, ADRD odds were 33% lower compared to blacks using other statins combined with non-RAS-acting AHTs (OR = 0.672 (CI: 0.548-0.825, p<0.001)).
Among older Americans, use of pravastatin and rosuvastatin to treat hyperlipidemia is less common than use of simvastatin and atorvastatin, however, in combination with RAS-acting AHTs, particularly ARBs, they may be more effective at reducing risk of ADRD. The number of Americans with ADRD may be reduced with drug treatments for vascular health that also confer effects on ADRD.
高血脂和高血压是阿尔茨海默病和相关痴呆症(ADRD)的可改变风险因素。大约 25%的 65 岁以上的成年人同时使用抗高血压药物(AHTs)和他汀类药物来治疗这些疾病。尽管越来越多的证据表明他汀类药物和 AHTs 与较低的 ADRD 风险独立相关,但尚无关于不同药物类别组合和 ADRD 风险同时使用的证据。我们的主要目标是比较同时使用不同的他汀类药物和抗高血压药物组合与 ADRD 风险之间的关系。
在一项回顾性队列研究(2007-2014 年)中,我们分析了美国 694672 名同时使用他汀类药物和 AHTs 的医疗保险受益人(2017786 人年)。我们使用逻辑回归调整年龄、社会经济地位和合并症,量化了与同时使用不同的他汀类药物分子(阿托伐他汀、普伐他汀、罗苏伐他汀和辛伐他汀)和 AHT 药物类别(两种肾素-血管紧张素系统(RAS)作用的 AHTs、血管紧张素转换酶抑制剂(ACEIs)或血管紧张素 II 受体阻滞剂(ARBs)与非 RAS 作用的 AHTs)相关的 ADRD 诊断的发生率。
普伐他汀或罗苏伐他汀与 RAS 作用的 AHTs 联合使用可降低与任何他汀类药物与非 RAS 作用的 AHTs 联合使用相关的 ADRD 风险:ACEI+普伐他汀比值比(OR)=0.942(95%置信区间:0.899-0.986,p=0.011),ACEI+罗苏伐他汀 OR=0.841(95%置信区间:0.794-0.892,p<0.001),ARB+普伐他汀 OR=0.794(95%置信区间:0.748-0.843,p<0.001),ARB+罗苏伐他汀 OR=0.818(95%置信区间:0.765-0.874,p<0.001)。与与普伐他汀或罗苏伐他汀联合使用相比,与阿托伐他汀和辛伐他汀联合使用的 ARBs 降低风险的幅度较小,而 ACEI 则没有降低风险。在西班牙裔中,与非 RAS 作用的 AHTs 相比,没有任何一种他汀类药物和 RAS 作用的 AHTs 的组合能降低风险。在使用 ACEI+罗苏伐他汀的黑人中,ADRD 的几率比使用其他他汀类药物与非 RAS 作用的 AHTs 联合使用的黑人低 33%(OR=0.672(95%置信区间:0.548-0.825,p<0.001))。
在美国老年人中,使用普伐他汀和罗苏伐他汀治疗高血脂的情况比使用辛伐他汀和阿托伐他汀的情况更为常见,然而,与 RAS 作用的 AHTs 联合使用,特别是 ARBs,可能更能降低 ADRD 的风险。通过治疗血管健康的药物治疗,可能会降低美国 ADRD 的发病率,而这些药物也会对 ADRD 产生影响。