de Vries Hielke M, Ottenhof Sarah R, Rafael Tynisha S, van Werkhoven Erik, Pos Floris J, van Rhijn Bas W G, Moonen Luc M F, Graafland Niels, de Feijter Jeantine M, Schaake Eva E, Horenblas Simon, Brouwer Oscar R
Department of Urology, The Netherlands Cancer Institute - Antoni van Leeuwenhoek Hospital, Amsterdam, The Netherlands.
Department of Biostatistics, The Netherlands Cancer Institute - Antoni van Leeuwenhoek Hospital, Amsterdam, The Netherlands.
Eur Urol Open Sci. 2022 Dec 15;47:29-35. doi: 10.1016/j.euros.2022.11.005. eCollection 2023 Jan.
Penile cancer (PeCa) is rare, and the survival of patients with advanced disease remains poor. A better understanding of where treatment fails could aid the development of new treatment strategies.
To describe the disease course after pelvic lymph node (LN) treatment for PeCa.
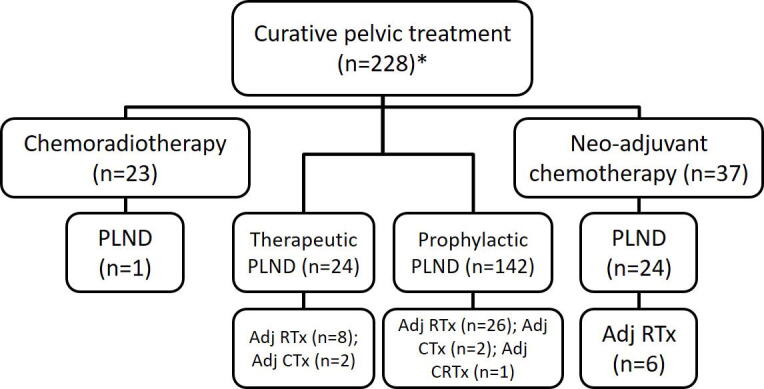
We retrospectively analysed 228 patients who underwent pelvic LN treatment with curative intent from 1969 to 2016. The main treatment modalities were neoadjuvant chemotherapy, chemoradiation, and pelvic LN dissection.
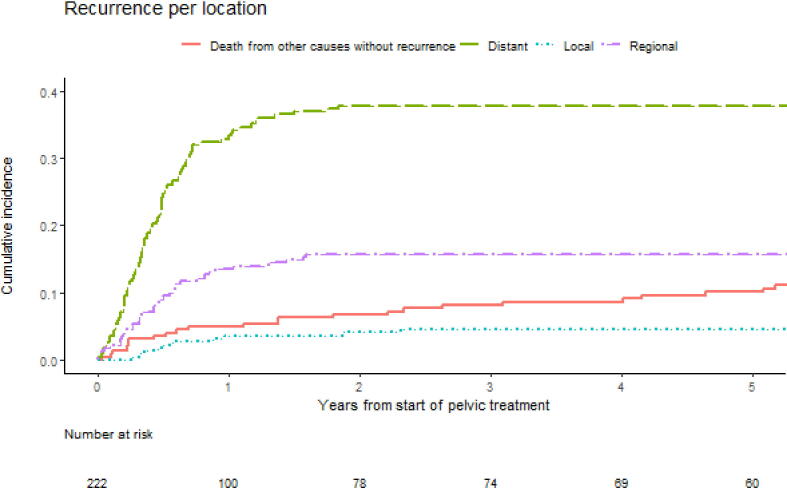
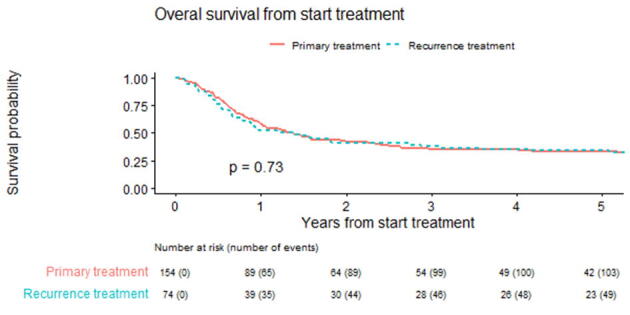
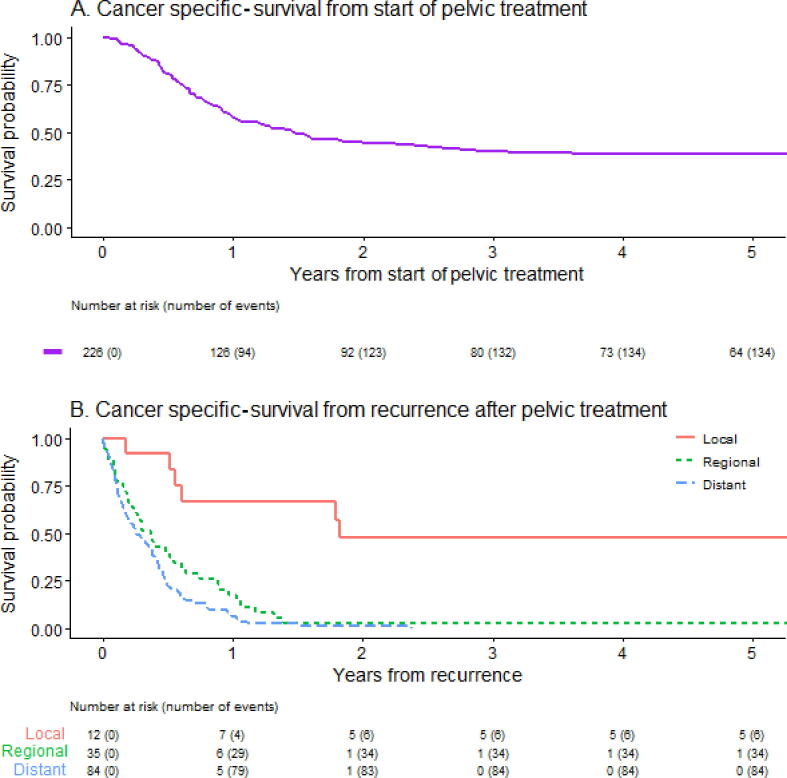
In the case of multiple recurrence locations, the most distant location was taken and recorded as follows: local (penis), regional (inguinal and pelvic LN), and distant (any other location). A competing risk analysis was used to calculate the time to recurrence per location, and a Kaplan-Meier analysis was used for overall survival (OS).
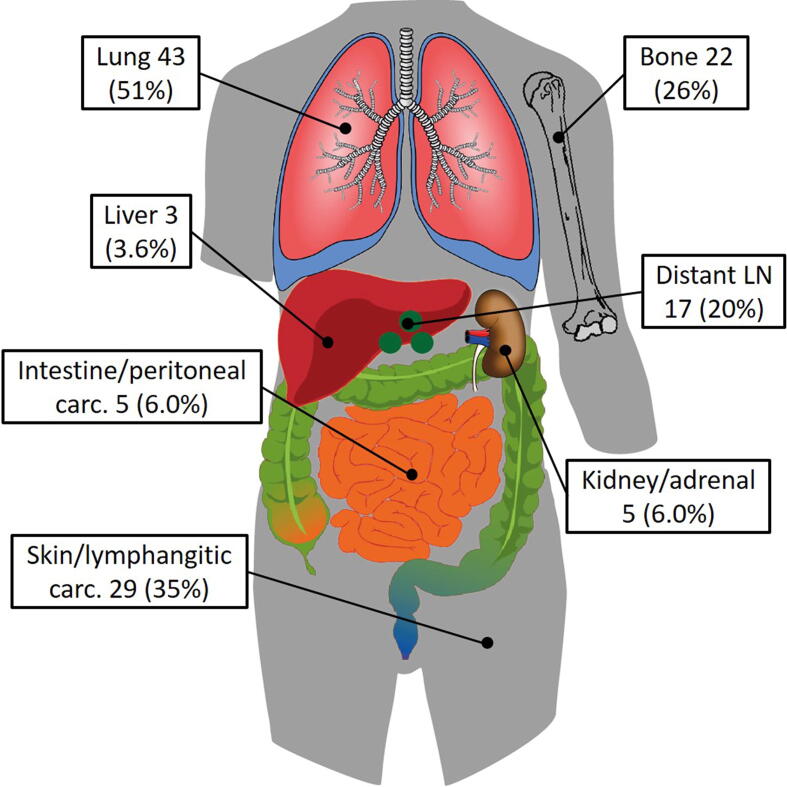
The median follow-up of the surviving patients was 79 mo. The reason for pelvic treatment was pelvic involvement on imaging (29%), two or more tumour-positive inguinal LNs (61%), or inguinal extranodal extension (52%). More than half of the patients (61%) developed a recurrence. The median recurrence-free survival was 11 mo. The distribution was local in 9%, regional in 27%, and distant in 64% of patients. The infield control rate of nonsystemically treated patients was 61% (113/184). From the start of pelvic treatment, the median OS was 17 mo (95% confidence interval 12-22). After regional or distant recurrence, all but one patient died of PeCa with median OS after a recurrence of 4.4 (regional) and 3.1 (distant) mo. This study is limited by its retrospective nature.
The prognosis of PeCa patients treated on their pelvis who recur despite locoregional treatment is poor. The tendency for systemic spread emphasises the need for more effective systemic treatment strategies.
In this report, we looked at the outcomes of penile cancer patients in an expert centre undergoing various treatments on their pelvis. We found that survival is poor after recurrence despite locoregional treatment. Therefore, better systemic treatments are necessary.
阴茎癌(PeCa)较为罕见,晚期疾病患者的生存率仍然很低。更好地了解治疗失败的部位有助于制定新的治疗策略。
描述阴茎癌盆腔淋巴结(LN)治疗后的疾病进程。
设计、地点和参与者:我们回顾性分析了1969年至2016年期间228例接受盆腔淋巴结根治性治疗的患者。主要治疗方式包括新辅助化疗、放化疗和盆腔淋巴结清扫术。
对于多个复发部位的情况,选取最远的部位并按以下方式记录:局部(阴茎)、区域(腹股沟和盆腔淋巴结)和远处(任何其他部位)。采用竞争风险分析计算每个部位的复发时间,采用Kaplan-Meier分析计算总生存期(OS)。
存活患者的中位随访时间为79个月。盆腔治疗的原因是影像学检查发现盆腔受累(29%)、两个或更多肿瘤阳性腹股沟淋巴结(61%)或腹股沟结外扩展(52%)。超过一半的患者(61%)出现复发。无复发生存期的中位数为11个月。患者复发部位分布为局部9%、区域27%、远处64%。未接受全身治疗患者的野内控制率为61%(113/184)。从盆腔治疗开始,中位总生存期为17个月(95%置信区间12 - 22)。区域或远处复发后,除1例患者外,所有患者均死于阴茎癌,复发后的中位总生存期为4.4个月(区域复发)和3.1个月(远处复发)。本研究受其回顾性性质的限制。
尽管进行了局部区域治疗,但盆腔接受治疗的阴茎癌患者复发后的预后较差。全身扩散的趋势强调了需要更有效的全身治疗策略。
在本报告中,我们观察了一家专家中心接受盆腔各种治疗的阴茎癌患者的结局。我们发现,尽管进行了局部区域治疗,但复发后的生存率很低。因此,需要更好的全身治疗方法。