Department of Orthopedics, The Second Affiliated Hospital of Nanchang University, No. 1 Minde Road, Nanchang, 330006, Jiangxi Province, China.
Department of Gastrointestinal Surgery, The First Affiliated Hospital of Nanchang University, Nanchang, China.
J Orthop Surg Res. 2023 Jan 5;18(1):13. doi: 10.1186/s13018-022-03490-x.
External fixators (EFs) and intramedullary nailing (IMN) are two effective methods for open tibial fractures. However, both methods have advantages and disadvantages, and the optimal surgical approach remains controversial. Thus, we performed a meta-analysis of randomized controlled trials (RCTs) to compare EF with IMN to evaluate their efficacy and safety.
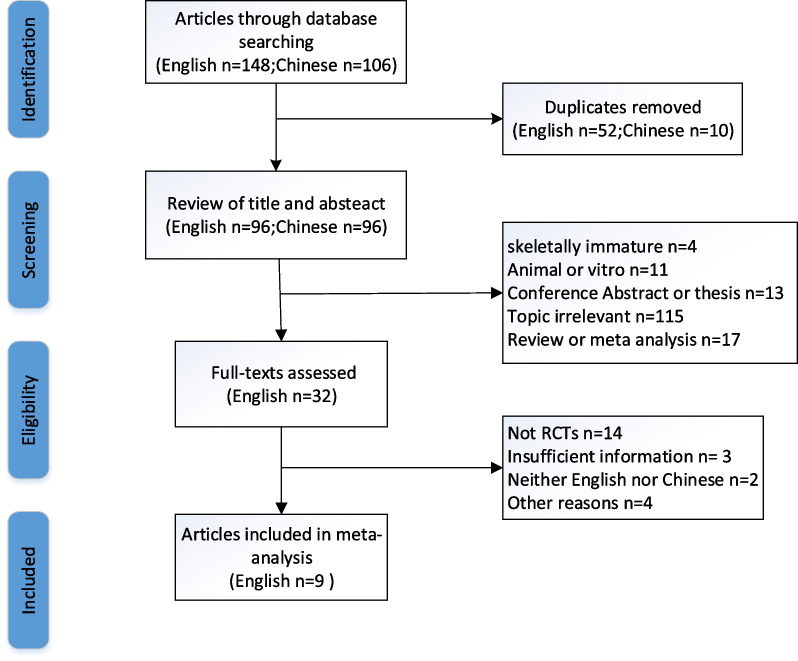
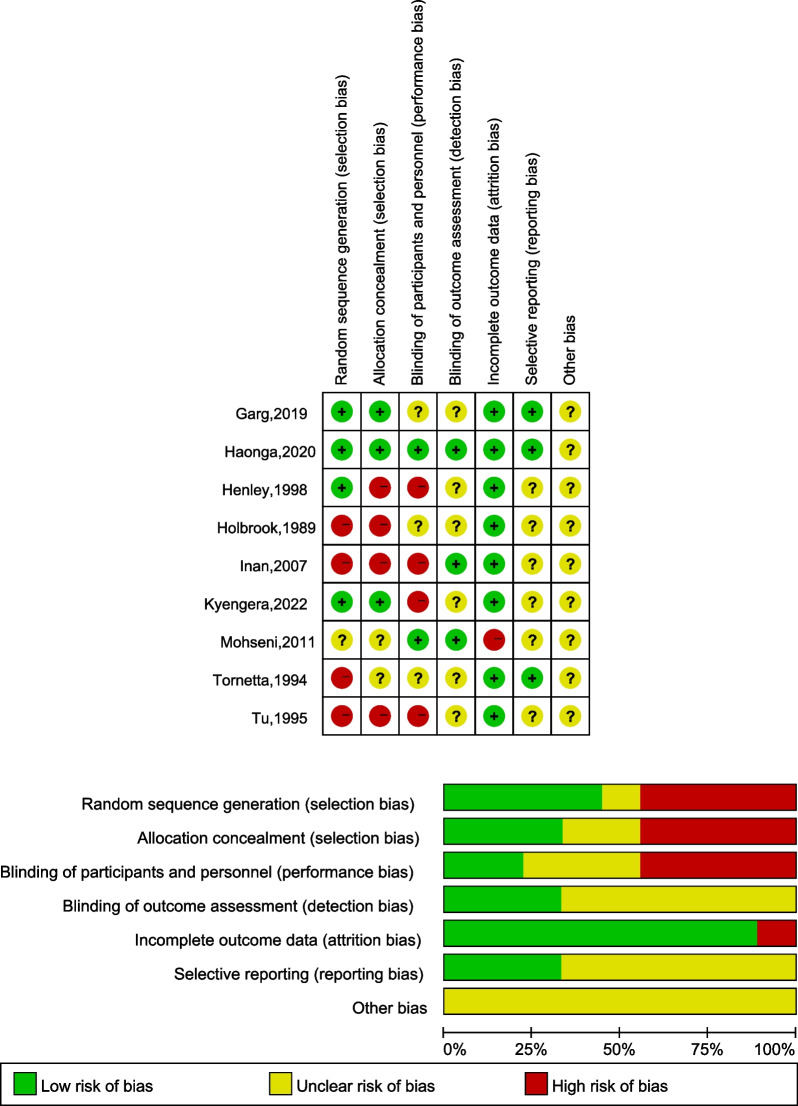
A systematic study of the literature was conducted in relevant studies published in PubMed, Embase, the Cochrane Library, Web of Science, CNKI, CBM, Wanfang and Weipu from database inception to April 2022. All eligible literature was critically appraised for methodological quality via the Cochrane's collaboration tool. The primary outcome measurements included postoperative superficial infection, postoperative deep infection, union time, delayed union, malunion, nonunion, and hardware failure.
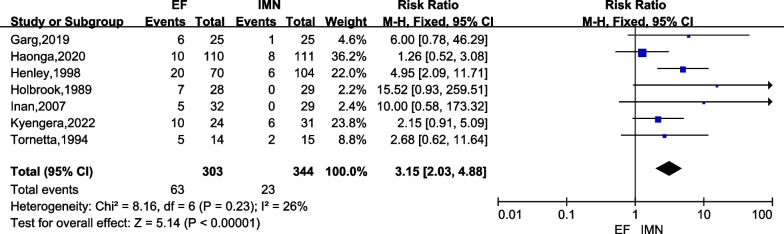
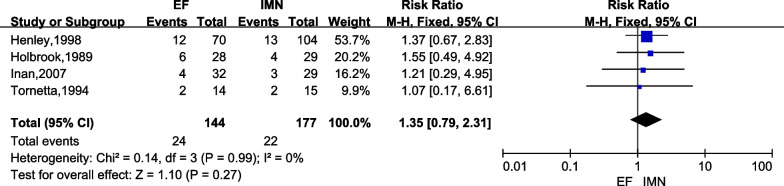
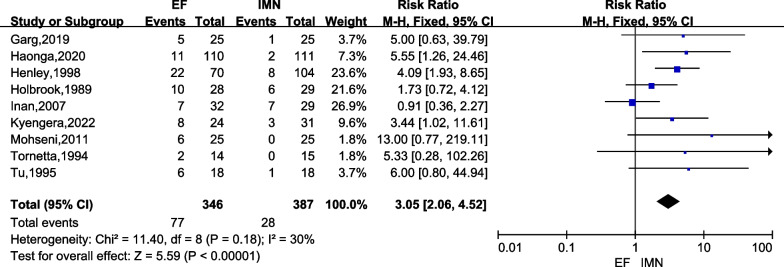
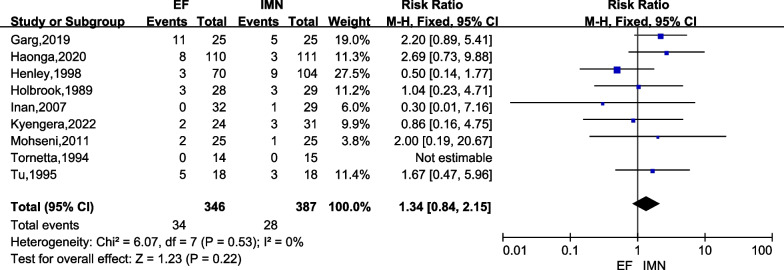
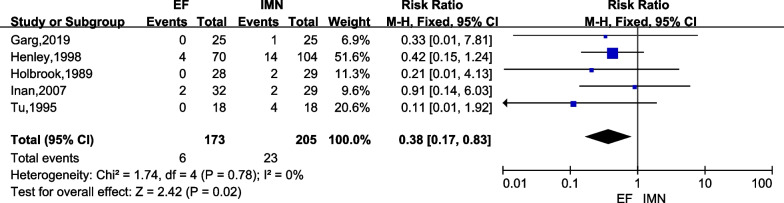
Nine RCTs involving 733 cases were included in the current meta-analysis. The pooled results suggested that cases in the IMN group had a significantly lower postoperative superficial infection rate [risk ratio (RR) = 2.84; 95% confidence interval (CI) = 1.83 to 4.39; P < 0.00001)] and malunion rate (RR = 3.05; 95% CI = 2.06 to 4.52; P < 0.00001) versus EF, but IMN had a significantly higher hardware failure occurrence versus EF (RR = 0.38; 95% CI = 0.17 to 0.83; P = 0.02). There were no significant differences in the postoperative deep infection rate, union time, delayed union rate or nonunion rate between the two groups (p > 0.05).
Compared to EF, IMN had a significantly lower risk of postoperative superficial infection and malunion in patients with open tibial fractures. Meanwhile, IMN did not prolong the union time and increased the risk of the deep infection rate, delayed union rate and nonunion rate but had a higher hardware failure rate. The reanalysis of union time showed that it was significantly shorter in the IMN group than in the EF group after excluding the study with significant heterogeneity during sensitivity analysis. Therefore, IMN is recommended as a preferred method of fracture fixation for patients with open tibial fractures, but more attention should be given to the problem of hardware failure.
外固定架(EF)和髓内钉(IMN)是治疗开放性胫骨骨折的两种有效方法。然而,两种方法都有其优缺点,最佳手术方法仍存在争议。因此,我们对随机对照试验(RCT)进行了荟萃分析,比较 EF 与 IMN,以评估它们的疗效和安全性。
系统检索了从数据库建立到 2022 年 4 月发表在 PubMed、Embase、Cochrane 图书馆、Web of Science、CNKI、CBM、万方和维普的相关研究。使用 Cochrane 协作工具对所有符合条件的文献进行了方法学质量评估。主要结局测量包括术后浅表感染、术后深部感染、愈合时间、延迟愈合、畸形愈合、不愈合和内固定失败。
纳入了 9 项 RCT 共 733 例患者。荟萃分析结果表明,IMN 组术后浅表感染率[风险比(RR)=2.84;95%置信区间(CI)=1.83 至 4.39;P<0.00001]和畸形愈合率(RR=3.05;95%CI=2.06 至 4.52;P<0.00001)明显低于 EF 组,但 IMN 组内固定失败发生率明显高于 EF 组(RR=0.38;95%CI=0.17 至 0.83;P=0.02)。两组术后深部感染率、愈合时间、延迟愈合率和不愈合率无统计学差异(P>0.05)。
与 EF 相比,IMN 治疗开放性胫骨骨折患者的术后浅表感染和畸形愈合风险明显降低。同时,IMN 并不延长愈合时间,但增加了深部感染率、延迟愈合率和不愈合率的风险,且内固定失败率较高。对愈合时间的重新分析表明,在敏感性分析中排除具有显著异质性的研究后,IMN 组的愈合时间明显短于 EF 组。因此,建议将 IMN 作为开放性胫骨骨折患者骨折固定的首选方法,但应更加关注内固定失败的问题。