Department of Operational Research, Indian Council of Medical Research - National Institute for Research in Reproductive and Child Health, Mumbai, Maharashtra, India.
Department of Population Health Sciences, King's College London, Ex-Regional Resource Hub for Health Technology Assessment, Indian Council of Medical Research - National Institute for Research in Reproductive and Child Health, Mumbai, Maharashtra, India.
BMC Pregnancy Childbirth. 2023 Jan 6;23(1):9. doi: 10.1186/s12884-022-05308-4.
Postpartum hemorrhage (PPH) is the global leading cause of maternal mortality, affecting nearly 3 to 6 percent of all women giving birth in India. The World Health Organization (WHO) has updated its guidelines to recommend the early use of intravenous (IV) tranexamic acid (TXA) in addition to standard care for all diagnosed PPH cases. This study aimed to assess the cost-effectiveness of introducing TXA for PPH management in the Indian public health system.
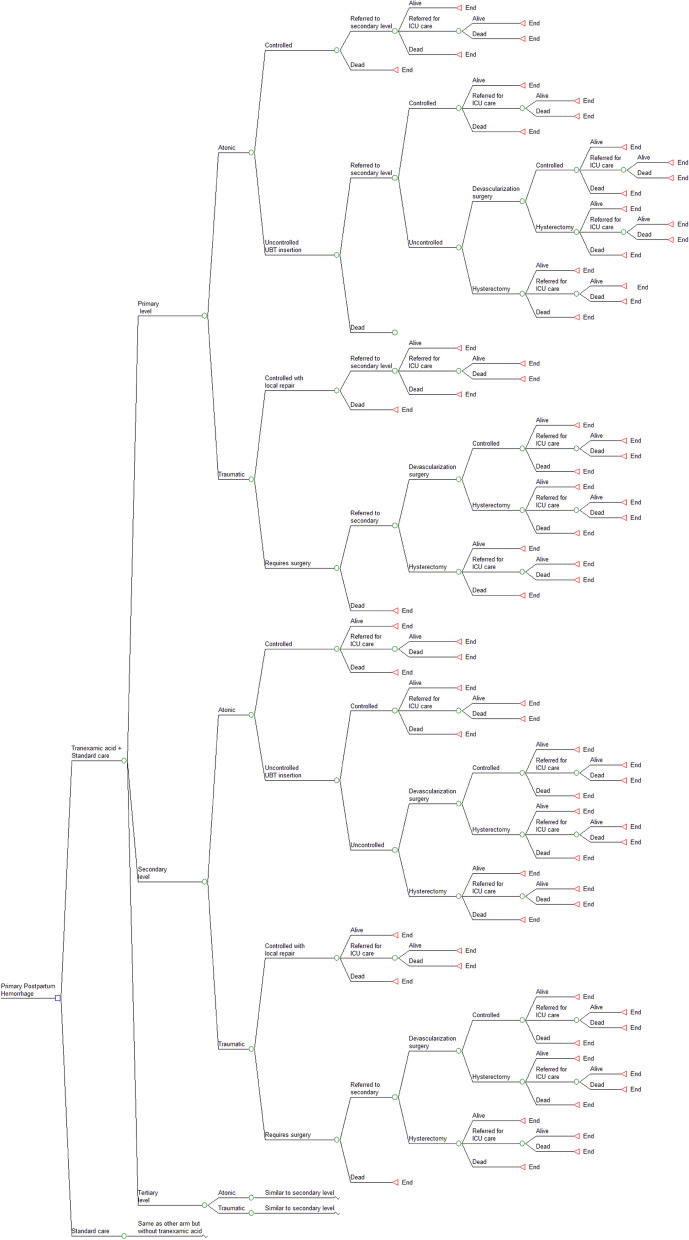
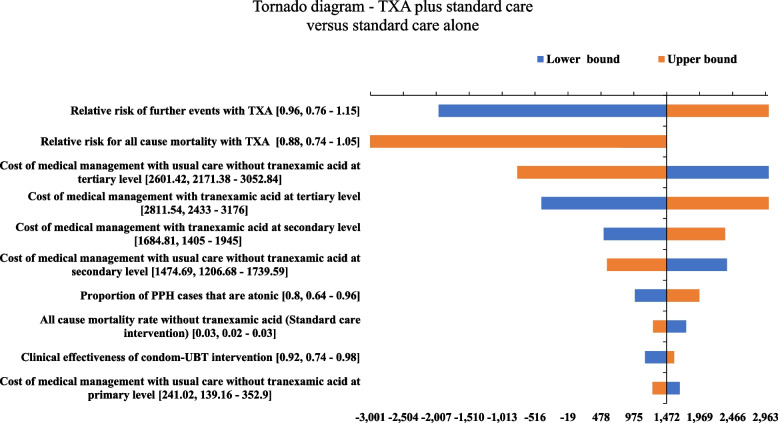
A decision analytic model was built using a decision tree to determine the cost-effectiveness of administering IV TXA to women experiencing PPH within 3 h of birth to existing management with uterotonics and supportive care. Using a disaggregated societal perspective, the costs and consequences for a hypothetical cohort of women experiencing PPH in public health facilities was estimated. The model was populated using probabilities, clinical parameters, and utilities from published literature, while cost parameters were largely derived from a primary economic costing study. The primary outcome of interest was the incremental cost-utility ratio (ICUR). Associated clinical events and net benefits were estimated. One-way and probabilistic sensitivity analysis (PSA) was undertaken. The budget impact was estimated for a national-level introduction.
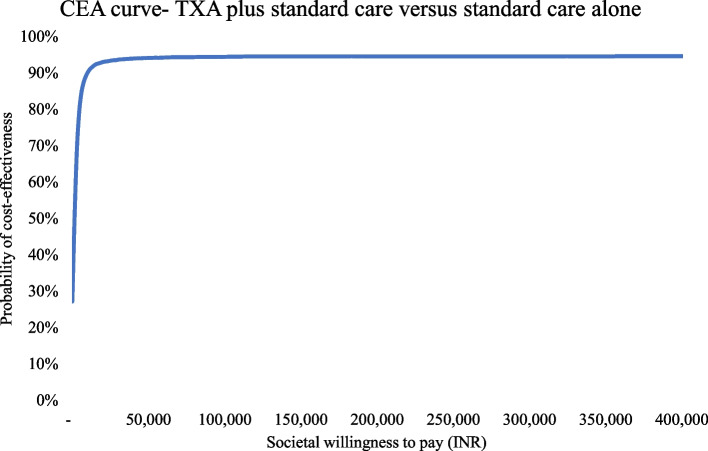
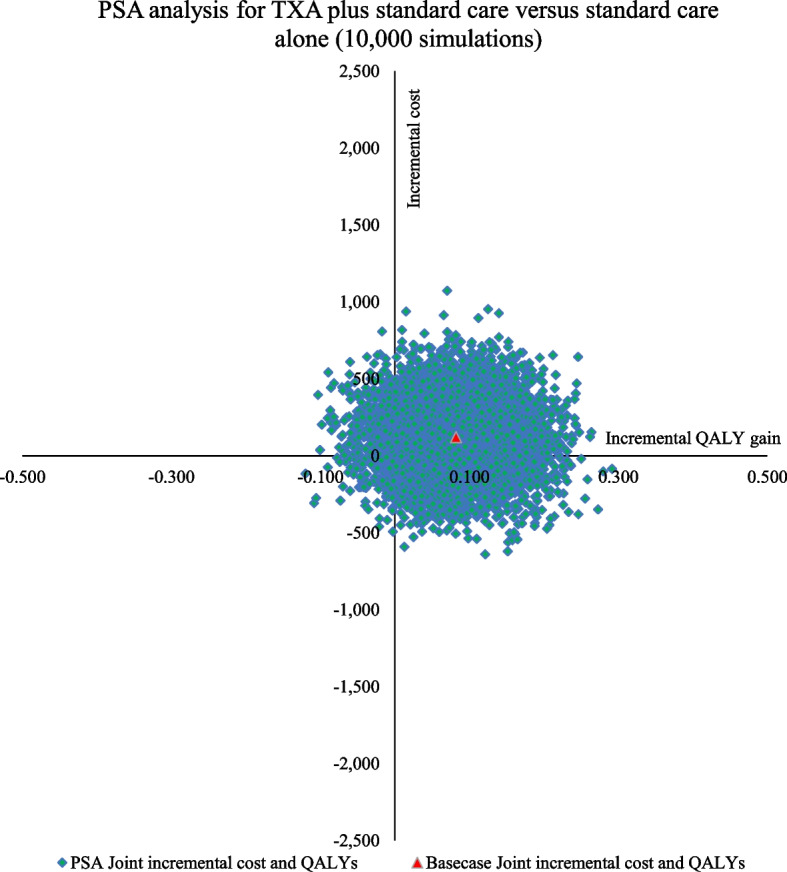
For an estimated annual cohort of 510,915 PPH cases in India, the addition of IV TXA would result in a per-patient disaggregated societal cost of INR 6607 (USD 95.15) with a discounted gain of 20.25 QALYs, as compared to a cost of INR 6486 (USD 93.41) with a discounted gain of 20.17 QALYs with standard care PPH management. At an ICUR value of INR 1470 per QALY gained (USD 21), the addition of IV TXA is cost-effective in Indian public health settings. The intervention is likely to prevent 389 maternal deaths, 177 surgeries, and 128 ICU admissions per 100,000 PPH cases. The findings are robust under uncertainty, with 94.5% of PSA simulations remaining cost-effective. A cumulative increase of 2.3% financial allocation for PPH management over five years will be incurred for TXA introduction.
Addition of tranexamic acid for primary PPH management, as recommended by WHO, is cost-effective in Indian public health settings. Policy guidelines, training manuals, and facility checklists should be updated to reflect this recommendation.
产后出血(PPH)是全球产妇死亡的主要原因,印度约有 3%至 6%的产妇受其影响。世界卫生组织(WHO)更新了其指南,建议对所有确诊的 PPH 病例在标准治疗的基础上,尽早使用静脉注射(IV)氨甲环酸(TXA)。本研究旨在评估在印度公共卫生系统中引入 TXA 治疗 PPH 的成本效益。
使用决策树构建决策分析模型,以确定在分娩后 3 小时内对经历 PPH 的妇女给予 IV TXA 与使用宫缩剂和支持性护理进行现有管理相比的成本效益。使用分解的社会视角,估计在公共卫生设施中经历 PPH 的假设妇女队列的成本和后果。模型使用来自已发表文献的概率、临床参数和效用进行填充,而成本参数主要来自一项主要的经济成本研究。主要结果是增量成本效益比(ICUR)。估计相关临床事件和净效益。进行了单因素和概率敏感性分析(PSA)。估计了在国家一级引入的预算影响。
对于印度每年估计的 510915 例 PPH 病例,与标准 PPH 管理相比,添加 IV TXA 将导致每位患者的社会分解成本增加 INR6607(95.15 美元),并获得折扣后的 20.25 QALY,而成本增加 INR6486(93.41 美元),获得折扣后的 20.17 QALY。在获得每 QALY 成本为 INR1470(21 美元)的情况下,IV TXA 在印度公共卫生环境中具有成本效益。该干预措施有望预防每 100000 例 PPH 中 389 例产妇死亡、177 例手术和 128 例 ICU 入院。在不确定性下,结果是稳健的,94.5%的 PSA 模拟结果仍然具有成本效益。在五年内,PPH 管理的财务拨款将增加 2.3%,用于 TXA 的引入。
按照世卫组织的建议,将 TXA 用于原发性 PPH 管理具有成本效益,可在印度公共卫生环境中实施。政策指南、培训手册和设施检查表应更新以反映这一建议。