Medicine & Emergency Medicine, Baylor College of Medicine, Houston, Texas, USA
Center for Research on Indigenous Health, Maya Health Alliance Wuqu' Kawoq, Tecpan, Guatemala.
BMJ Open. 2023 Jan 6;13(1):e056913. doi: 10.1136/bmjopen-2021-056913.
The burden of diabetes mellitus is increasing in low-income and middle-income countries (LMICs). Few studies have explored pathways to care among individuals with diabetes in LMICs. This study evaluates care trajectories among adults with diabetes in rural Guatemala.
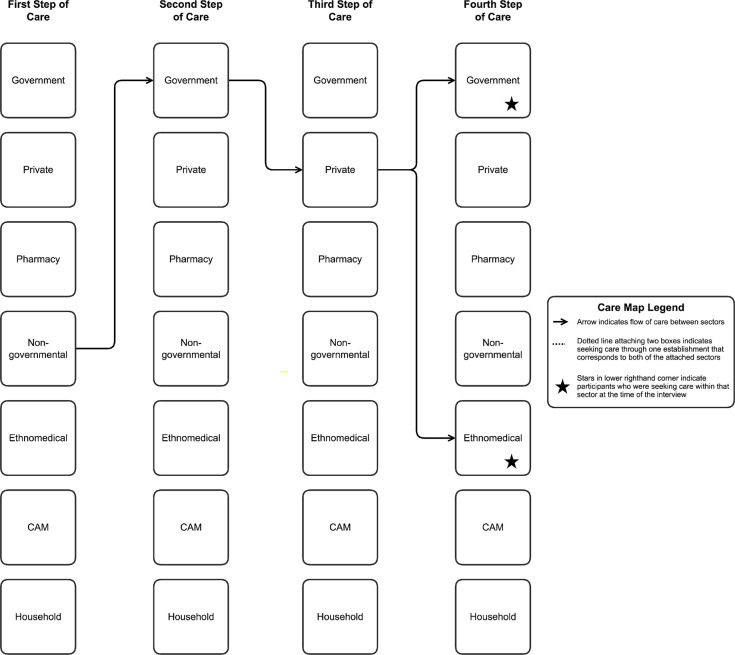
A qualitative investigation was conducted as part of a population-based study assessing incidence and risk factors for chronic kidney disease in two rural sites in Guatemala. A random sample of 807 individuals had haemoglobin A1c (HbA1c) screening for diabetes in both sites. Based on results from the first 6 months of the population study, semistructured interviews were performed with 29 adults found to have an HbA1c≥6.5% and who reported a previous diagnosis of diabetes. Interviews explored pathways to and experiences of diabetes care. Detailed interview notes were coded using NVivo and used to construct diagrams depicting each participant's pathway to care and use of distinct healthcare sectors.
Participants experienced fragmented care across multiple health sectors (97%), including government, private and non-governmental sectors. The majority of participants sought care with multiple providers for diabetes (90%), at times simultaneously and at times sequentially, and did not have longitudinal continuity of care with a single provider. Many participants experienced financial burden from out-of-pocket costs associated with diabetes care (66%) despite availability of free government sector care. Participants perceived government diabetes care as low-quality due to resource limitations and poor communication with providers, leading some to seek care in other health sectors.
This study highlights the fragmented, discontinuous nature of diabetes care in Guatemala across public, private and non-governmental health sectors. Strategies to improve diabetes care access in Guatemala and other LMICs should be multisectorial and occur through strengthened government primary care and innovative private and non-governmental organisation care models.
糖尿病在低收入和中等收入国家(LMICs)的负担正在增加。很少有研究探讨过 LMICs 中糖尿病患者的护理途径。本研究评估了危地马拉农村地区成年糖尿病患者的护理轨迹。
作为一项评估危地马拉两个农村地区慢性肾脏病发病率和危险因素的基于人群研究的一部分,进行了定性研究。在两个地点,对 807 名随机抽样的个体进行了血红蛋白 A1c(HbA1c)筛查,以确定糖尿病。根据人群研究的前 6 个月的结果,对 29 名 HbA1c≥6.5%且报告有糖尿病既往诊断的成年人进行了半结构化访谈。访谈探讨了寻求糖尿病护理的途径和经验。使用 NVivo 对详细的访谈记录进行编码,并用于构建描绘每个参与者的护理途径和使用不同医疗保健部门的图表。
参与者在多个卫生部门(97%)经历了零碎的护理,包括政府、私营和非政府部门。大多数参与者因糖尿病护理相关的自付费用(66%)而经历了经济负担,尽管政府部门提供了免费的护理。由于资源限制和与提供者沟通不畅,参与者认为政府的糖尿病护理质量较低,这导致一些人在其他卫生部门寻求护理。
本研究强调了危地马拉公共、私人和非政府卫生部门在糖尿病护理方面的零碎、不连续的性质。改善危地马拉和其他 LMICs 糖尿病护理获取的策略应该是多部门的,并通过加强政府初级保健和创新的私人和非政府组织护理模式来实现。