Internal Medicine Residency Program, UPMC Mercy, Pittsburgh, Pennsylvania, USA.
Division of Pulmonary, Critical Care, and Sleep Medicine, MetroHealth Medical Center, Cleveland, Ohio, USA.
BMJ Open. 2023 Jan 12;13(1):e066626. doi: 10.1136/bmjopen-2022-066626.
To reliably quantify the radiographic severity of COVID-19 pneumonia with the Radiographic Assessment of Lung Edema (RALE) score on clinical chest X-rays among inpatients and examine the prognostic value of baseline RALE scores on COVID-19 clinical outcomes.
Hospitalised patients with COVID-19 in dedicated wards and intensive care units from two different hospital systems.
425 patients with COVID-19 in a discovery data set and 415 patients in a validation data set.
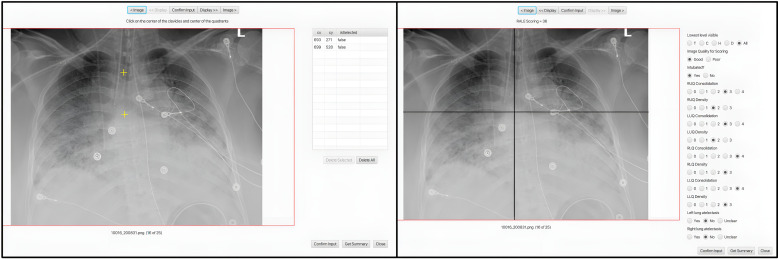
We measured inter-rater reliability for RALE score annotations by different reviewers and examined for associations of consensus RALE scores with the level of respiratory support, demographics, physiologic variables, applied therapies, plasma host-response biomarkers, SARS-CoV-2 RNA load and clinical outcomes.
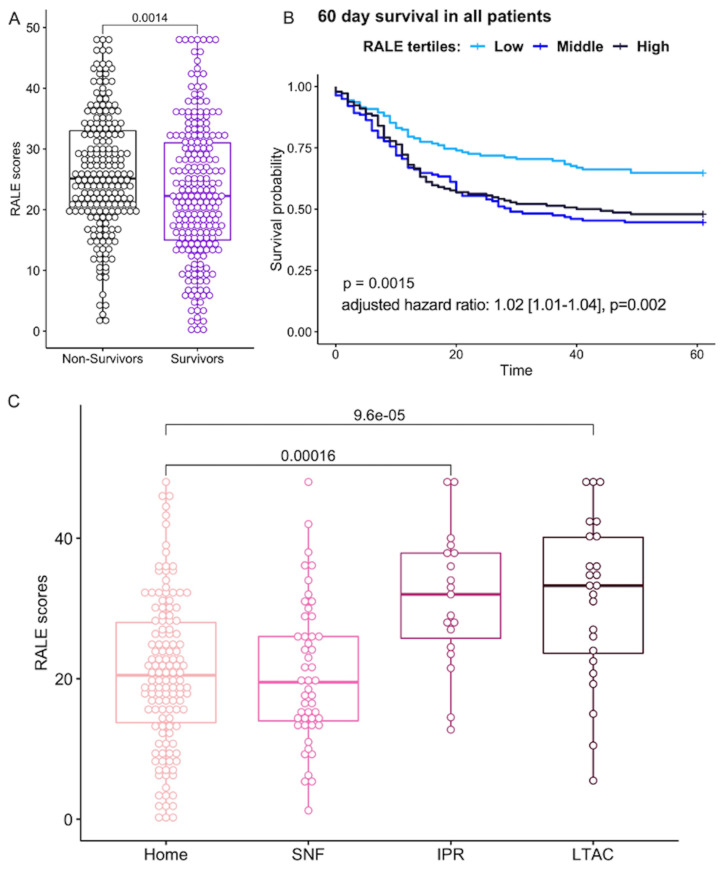
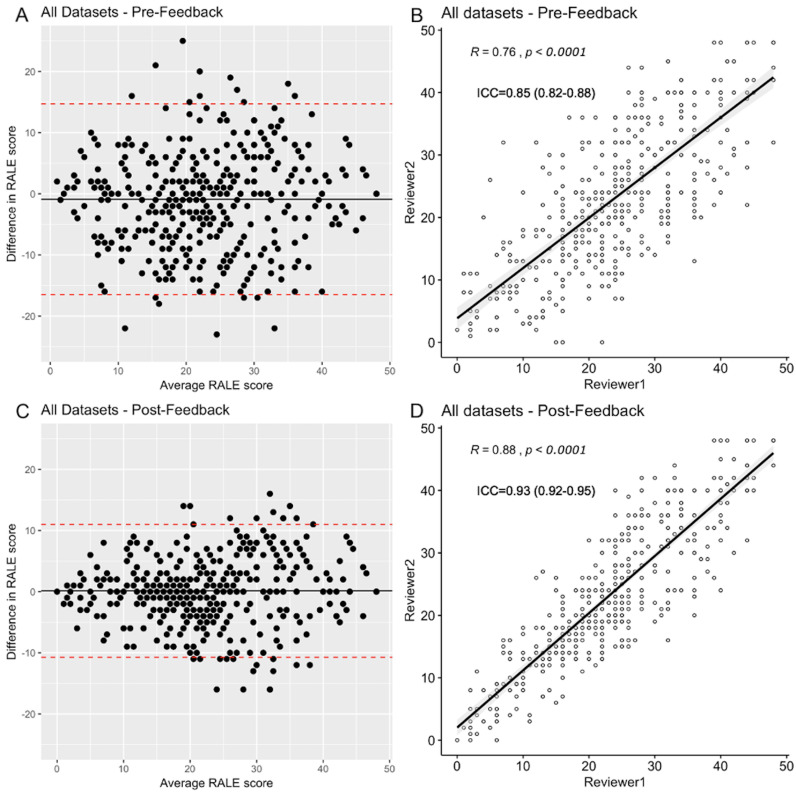
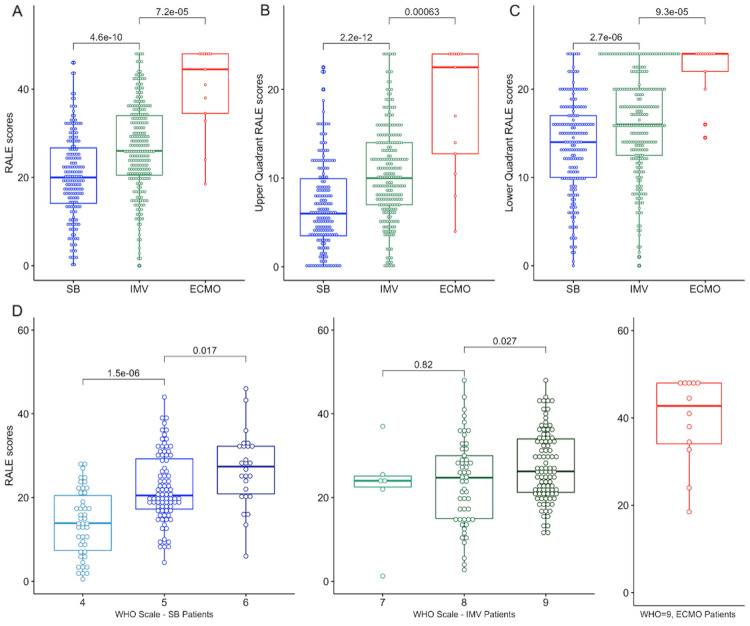
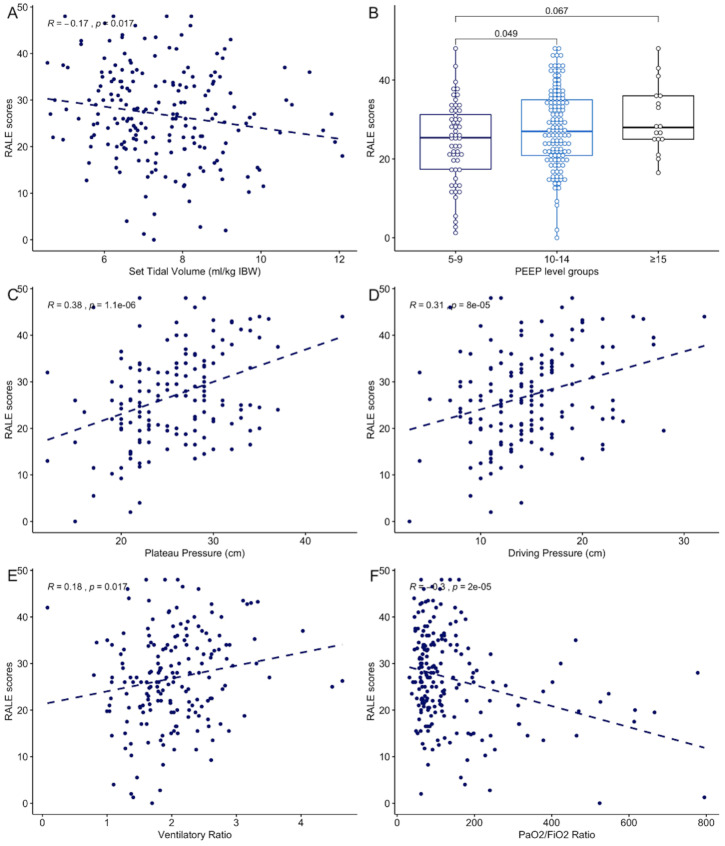
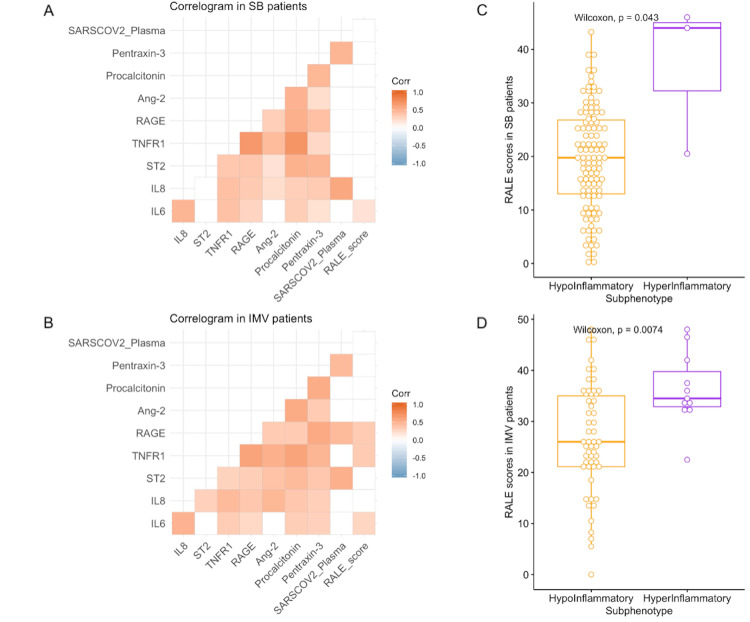
Inter-rater agreement for RALE scores improved from fair to excellent following reviewer training and feedback (intraclass correlation coefficient of 0.85 vs 0.93, respectively). In the discovery cohort, the required level of respiratory support at the time of CXR acquisition (supplemental oxygen or non-invasive ventilation (n=178); invasive-mechanical ventilation (n=234), extracorporeal membrane oxygenation (n=13)) was significantly associated with RALE scores (median (IQR): 20.0 (14.1-26.7), 26.0 (20.5-34.0) and 44.5 (34.5-48.0), respectively, p<0.0001). Among invasively ventilated patients, RALE scores were significantly associated with worse respiratory mechanics (plateau and driving pressure) and gas exchange metrics (PaO2/FiO2 and ventilatory ratio), as well as higher plasma levels of IL-6, soluble receptor of advanced glycation end-products and soluble tumour necrosis factor receptor 1 (p<0.05). RALE scores were independently associated with 90-day survival in a multivariate Cox proportional hazards model (adjusted HR 1.04 (1.02-1.07), p=0.002). We replicated the significant associations of RALE scores with baseline disease severity and mortality in the independent validation data set.
With a reproducible method to measure radiographic severity in COVID-19, we found significant associations with clinical and physiologic severity, host inflammation and clinical outcomes. The incorporation of radiographic severity assessments in clinical decision-making may provide important guidance for prognostication and treatment allocation in COVID-19.
通过对来自两个不同医院系统的专门病房和重症监护病房的住院 COVID-19 患者的临床胸部 X 光片,使用放射学肺水肿评估(RALE)评分可靠地量化 COVID-19 肺炎的放射学严重程度,并检查基线 RALE 评分对 COVID-19 临床结局的预后价值。
来自两个不同医院系统的专门病房和重症监护病房的住院 COVID-19 患者。
发现数据集的 425 名 COVID-19 患者和验证数据集的 415 名患者。
我们通过不同的审阅者测量了 RALE 评分注释的组内可靠性,并检查了共识 RALE 评分与呼吸支持水平、人口统计学、生理变量、应用治疗方法、血浆宿主反应生物标志物、SARS-CoV-2 RNA 载量和临床结局之间的关联。
在审阅者培训和反馈后,RALE 评分的组内一致性从一般提高到优秀(组内相关系数分别为 0.85 和 0.93)。在发现队列中,CXR 采集时所需的呼吸支持水平(补充氧气或无创通气(n=178);有创机械通气(n=234);体外膜氧合(n=13))与 RALE 评分显著相关(中位数(IQR):20.0(14.1-26.7)、26.0(20.5-34.0)和 44.5(34.5-48.0),p<0.0001)。在有创通气的患者中,RAL 评分与较差的呼吸力学(平台压和驱动压)和气体交换指标(PaO2/FiO2 和通气比)以及更高的血浆 IL-6、晚期糖基化终产物可溶性受体和可溶性肿瘤坏死因子受体 1 水平显著相关(p<0.05)。在多变量 Cox 比例风险模型中,RAL 评分与 90 天生存率独立相关(调整后的 HR 1.04(1.02-1.07),p=0.002)。我们在独立验证数据集中复制了 RALE 评分与基线疾病严重程度和死亡率的显著相关性。
使用一种可重复的方法来测量 COVID-19 的放射学严重程度,我们发现与临床和生理严重程度、宿主炎症和临床结局显著相关。在临床决策中纳入放射学严重程度评估可能为 COVID-19 的预后和治疗分配提供重要指导。