Division of Cardiovascular Medicine, Stanford University School of Medicine, Stanford, California.
Azienda Ospedaliera Universitaria Careggi, Florence, Italy.
JAMA Cardiol. 2023 Mar 1;8(3):240-247. doi: 10.1001/jamacardio.2022.5099.
Mavacamten, a cardiac myosin inhibitor, improved peak oxygen uptake (pVO2) in patients with symptomatic obstructive hypertrophic cardiomyopathy (HCM) in the EXPLORER-HCM study. However, the full extent of mavacamten's effects on exercise performance remains unclear.
To investigate the effect of mavacamten on exercise physiology using cardiopulmonary exercise testing (CPET).
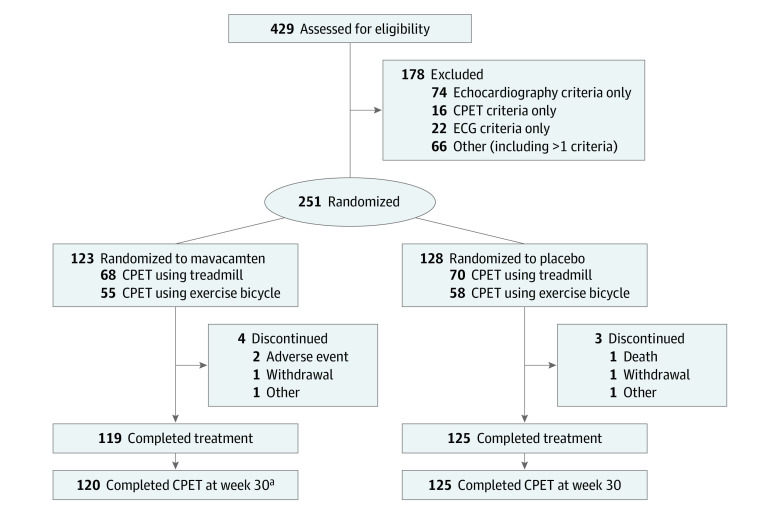
DESIGN, SETTING, AND PARTICIPANTS: Exploratory analyses of the data from the EXPLORER-HCM study, a randomized, double-blind, placebo-controlled, phase 3 trial that was conducted in 68 cardiovascular centers in 13 countries. In total, 251 patients with symptomatic obstructive HCM were enrolled.
Patients were randomly assigned in a 1:1 ratio to mavacamten or placebo.
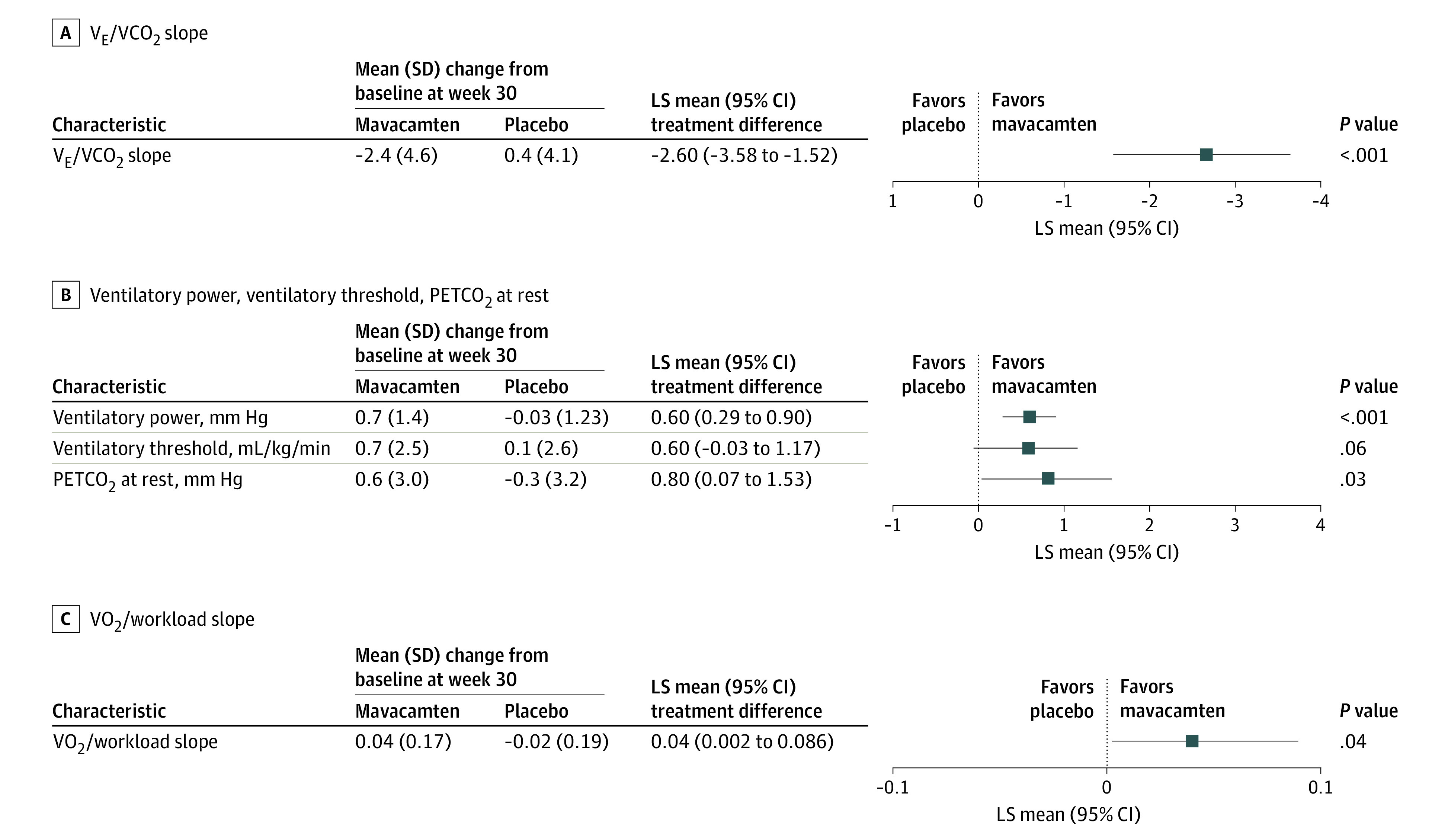
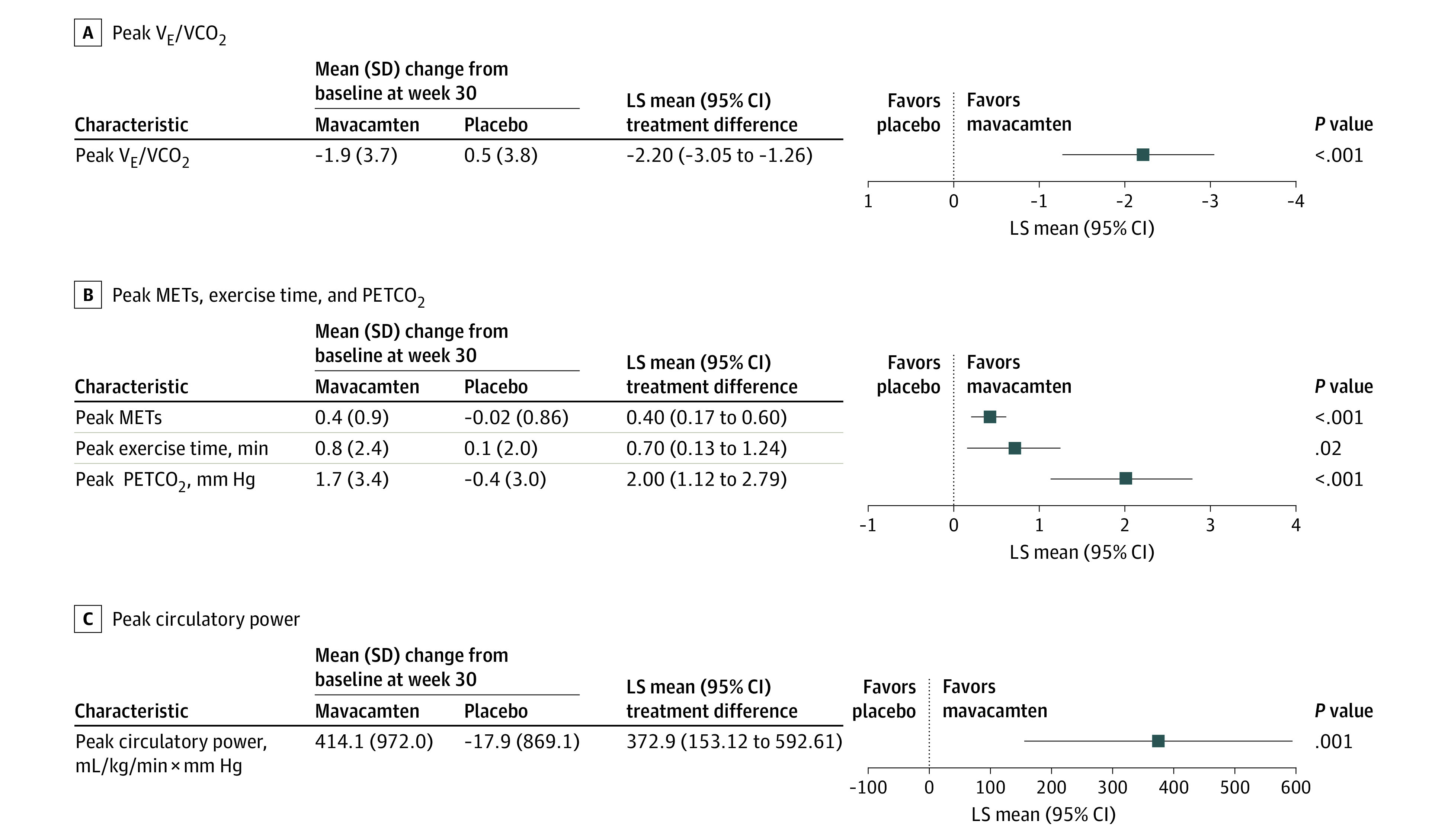
The following prespecified exploratory cardiovascular and performance parameters were assessed with a standardized treadmill or bicycle ergometer test protocol at baseline and week 30: carbon dioxide output (VCO2), minute ventilation (VE), peak VE/VCO2 ratio, ventilatory efficiency (VE/VCO2 slope), peak respiratory exchange ratio (RER), peak circulatory power, ventilatory power, ventilatory threshold, peak metabolic equivalents (METs), peak exercise time, partial pressure of end-tidal carbon dioxide (PETCO2), and VO2/workload slope.
Two hundred fifty-one patients were enrolled. The mean (SD) age was 58.5 (11.9) years and 59% of patients were male. There were significant improvements with mavacamten vs placebo in the following peak-exercise CPET parameters: peak VE/VCO2 ratio (least squares [LS] mean difference, -2.2; 95% CI, -3.05 to -1.26; P < .001), peak METs (LS mean difference, 0.4; 95% CI, 0.17-0.60; P < .001), peak circulatory power (LS mean difference, 372.9 mL/kg/min × mm Hg; 95% CI, 153.12-592.61; P = .001), and peak PETCO2 (LS mean difference, 2.0 mm Hg; 95% CI, 1.12-2.79; P < .001). Mavacamten also improved peak exercise time compared with placebo (LS mean difference, 0.7 minutes; 95% CI, 0.13-1.24; P = .02). There was a significant improvement in nonpeak-exercise CPET parameters, such as VE/VCO2 slope (LS mean difference, -2.6; 95% CI, -3.58 to -1.52; P < .001) and ventilatory power (LS mean difference, 0.6 mm Hg; 95% CI, 0.29-0.90; P < .001) favoring mavacamten vs placebo.
Mavacamten improved a range of CPET parameters beyond pVO2, indicating consistent and broad benefits on maximal exercise capacity. Although improvements in peak-exercise CPET parameters are clinically meaningful, the favorable effects of mavacamten on submaximal exertional tolerance provide further insights into the beneficial impact of mavacamten in patients with obstructive HCM.
ClinicalTrials.gov Identifier: NCT03470545.
心肌肌球蛋白抑制剂马卡塞坦可改善有症状梗阻性肥厚型心肌病(HCM)患者的峰值摄氧量(pVO2),这在 EXPLORER-HCM 研究中得到了证实。然而,马卡塞坦对运动表现的全面影响仍不清楚。
通过心肺运动测试(CPET)研究马卡塞坦对运动生理学的影响。
设计、地点和参与者:对来自 EXPLORER-HCM 研究的数据进行探索性分析,该研究是在 13 个国家的 68 个心血管中心进行的一项随机、双盲、安慰剂对照、3 期试验。共纳入 251 例有症状梗阻性 HCM 患者。
患者以 1:1 的比例随机分配至马卡塞坦或安慰剂组。
在基线和第 30 周时,采用标准化跑步机或自行车测力计测试方案评估以下预设的心血管和性能参数:二氧化碳输出(VCO2)、分钟通气量(VE)、峰值 VE/VCO2 比值、通气效率(VE/VCO2 斜率)、峰值呼吸交换率(RER)、峰值循环功率、通气功率、通气阈、峰值代谢当量(METs)、峰值运动时间、呼气末二氧化碳分压(PETCO2)和 VO2/负荷斜率。
共纳入 251 例患者。患者的平均(SD)年龄为 58.5(11.9)岁,59%的患者为男性。与安慰剂相比,马卡塞坦在以下峰值运动 CPET 参数中具有显著改善:峰值 VE/VCO2 比值(最小二乘[LS]均值差异,-2.2;95%CI,-3.05 至-1.26;P < .001)、峰值 METs(LS 均值差异,0.4;95%CI,0.17-0.60;P < .001)、峰值循环功率(LS 均值差异,372.9 mL/kg/min×mmHg;95%CI,153.12-592.61;P = .001)和峰值 PETCO2(LS 均值差异,2.0 mmHg;95%CI,1.12-2.79;P < .001)。与安慰剂相比,马卡塞坦还改善了峰值运动时间(LS 均值差异,0.7 分钟;95%CI,0.13-1.24;P =.02)。非峰值运动 CPET 参数也有显著改善,如 VE/VCO2 斜率(LS 均值差异,-2.6;95%CI,-3.58 至-1.52;P < .001)和通气功率(LS 均值差异,0.6 mmHg;95%CI,0.29-0.90;P < .001),均有利于马卡塞坦。
马卡塞坦改善了一系列 CPET 参数,除了 pVO2 之外,这表明其对最大运动能力有一致和广泛的益处。尽管峰值运动 CPET 参数的改善具有临床意义,但马卡塞坦对亚最大运动耐力的有利影响进一步深入了解了马卡塞坦对梗阻性 HCM 患者的有益影响。
ClinicalTrials.gov 标识符:NCT03470545。