Xie Yuxue, Li Xiangwen, Liu Shaohua, Hu Yiwen, Chen Ye, Liu Shiyin, Wu Puye, Tao Hongyue, Chen Shuang
Department of Radiology and Institute of Medical Functional and Molecular Imaging, Huashan Hospital, Fudan University, Shanghai, China.
Department of Sports Medicine, Huashan Hospital, Fudan University, Shanghai, China.
Orthop J Sports Med. 2023 Jan 11;11(1):23259671221137835. doi: 10.1177/23259671221137835. eCollection 2023 Jan.
Rotator cuff retears occur more often at the proximal region with the suture-bridge (SB) technique than at the typical footprint region with the single-row (SR) technique. Few longitudinal clinical trials have focused on the postoperative tendon quality of the repaired rotator cuff at different regions between the 2 techniques.
To compare tendon healing of the proximal and distal regions between the SB and SR techniques.
Cohort study; Level of evidence, 3.
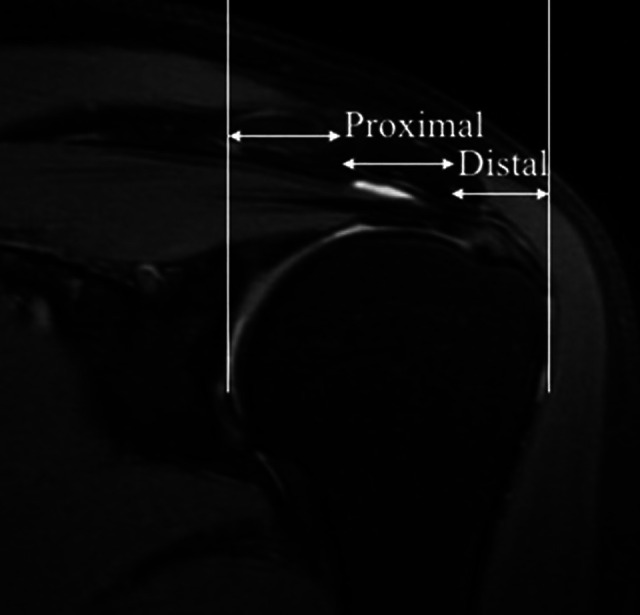
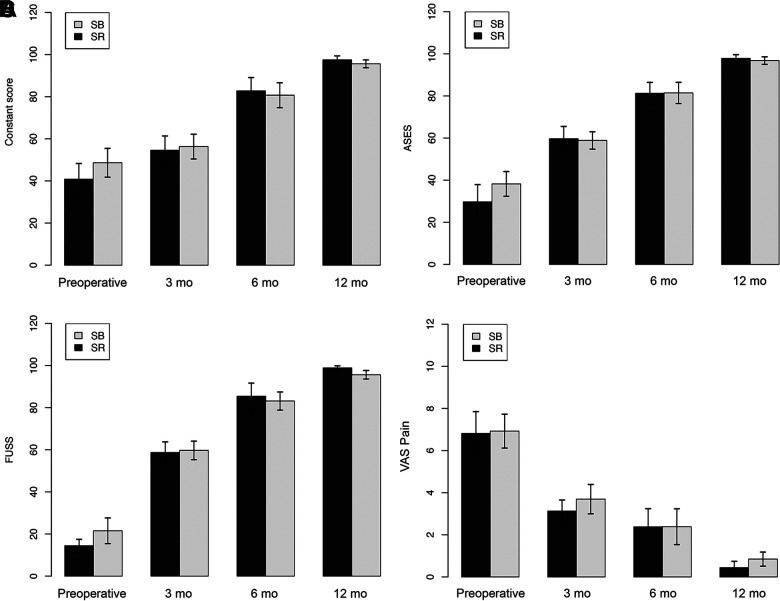
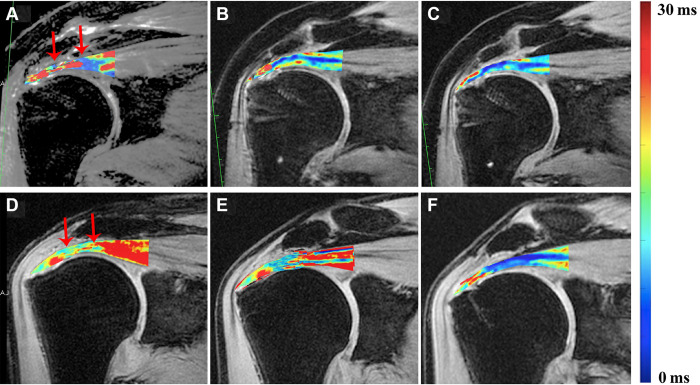
Included were consecutive patients who underwent arthroscopic rotator cuff repair and undertook clinical and magnetic resonance imaging (MRI) examinations at 3, 6, and 12 months postoperatively between 2016 and 2017. These patients were divided into the SB and SR groups according to the technique used. The repaired tendon was segmented into distal and proximal regions on ultrashort echo time-T2* mapping images. Clinical outcomes (Constant score, American Shoulder and Elbow Surgeons score, Fudan University Shoulder Score, and visual analog scale for pain) and MRI-based tendon healing (T2* values) of different regions were compared between the 2 groups. The differences in T2* values and clinical scores were determined by 1-way analysis of variance for repeated measurements.
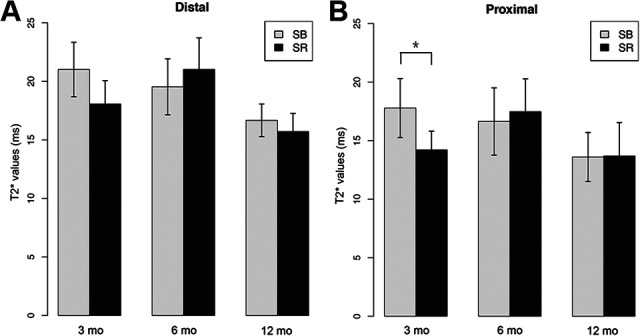
A total of 31 patients (17 in SB group and 14 in SR group) were included. At 12-month follow-up, significant improvements from preoperatively were achieved for all patients in all clinical scores ( < .001 for all). No significant between-group differences were found in T2* values of the distal region at any time point; however, the mean T2* value of the proximal region at 3 months was significantly higher in the SB group compared with the SR group ( = .03). This difference became nonsignificant at subsequent follow-up time points.
Significant clinical improvements over time can be expected in the first year after arthroscopic rotator cuff repair. In the early postoperative period, higher T2* values in the proximal region of the repaired tendon (representing inferior tendon quality) were seen with the SB technique compared with the SR technique; however, this phenomenon was resolved over time.
与采用单排(SR)技术在典型的肌腱附着区相比,采用缝线桥(SB)技术时肩袖 retears 在近端区域更常发生。很少有纵向临床试验关注这两种技术在不同区域修复后的肩袖肌腱质量。
比较 SB 技术和 SR 技术在近端和远端区域的肌腱愈合情况。
队列研究;证据等级,3 级。
纳入 2016 年至 2017 年间接受关节镜下肩袖修复并在术后 3、6 和 12 个月进行临床和磁共振成像(MRI)检查的连续患者。根据所使用的技术将这些患者分为 SB 组和 SR 组。在超短回波时间 - T2* 映射图像上,将修复的肌腱分为远端和近端区域。比较两组不同区域的临床结果(Constant 评分、美国肩肘外科医师评分、复旦大学肩部评分和疼痛视觉模拟量表)和基于 MRI 的肌腱愈合情况(T2* 值)。T2* 值和临床评分的差异通过重复测量的单因素方差分析确定。
共纳入 31 例患者(SB 组 17 例,SR 组 14 例)。在 12 个月的随访中,所有患者的所有临床评分与术前相比均有显著改善(所有 P <.001)。在任何时间点,远端区域的 T2* 值在组间均未发现显著差异;然而,SB 组在 3 个月时近端区域的平均 T2* 值显著高于 SR 组(P =.03)。在随后的随访时间点,这种差异变得不显著。
关节镜下肩袖修复术后第一年,随着时间推移临床可预期有显著改善。在术后早期,与 SR 技术相比,SB 技术修复的肌腱近端区域 T2* 值较高(代表肌腱质量较差);然而,这种现象随时间得到解决。